Chapter: Medical Microbiology: An Introduction to Infectious Diseases: Mycobacteria
Mycobacteria Causing Tuberculosis-Like Diseases
MYCOBACTERIA CAUSING TUBERCULOSIS-LIKE DISEASES
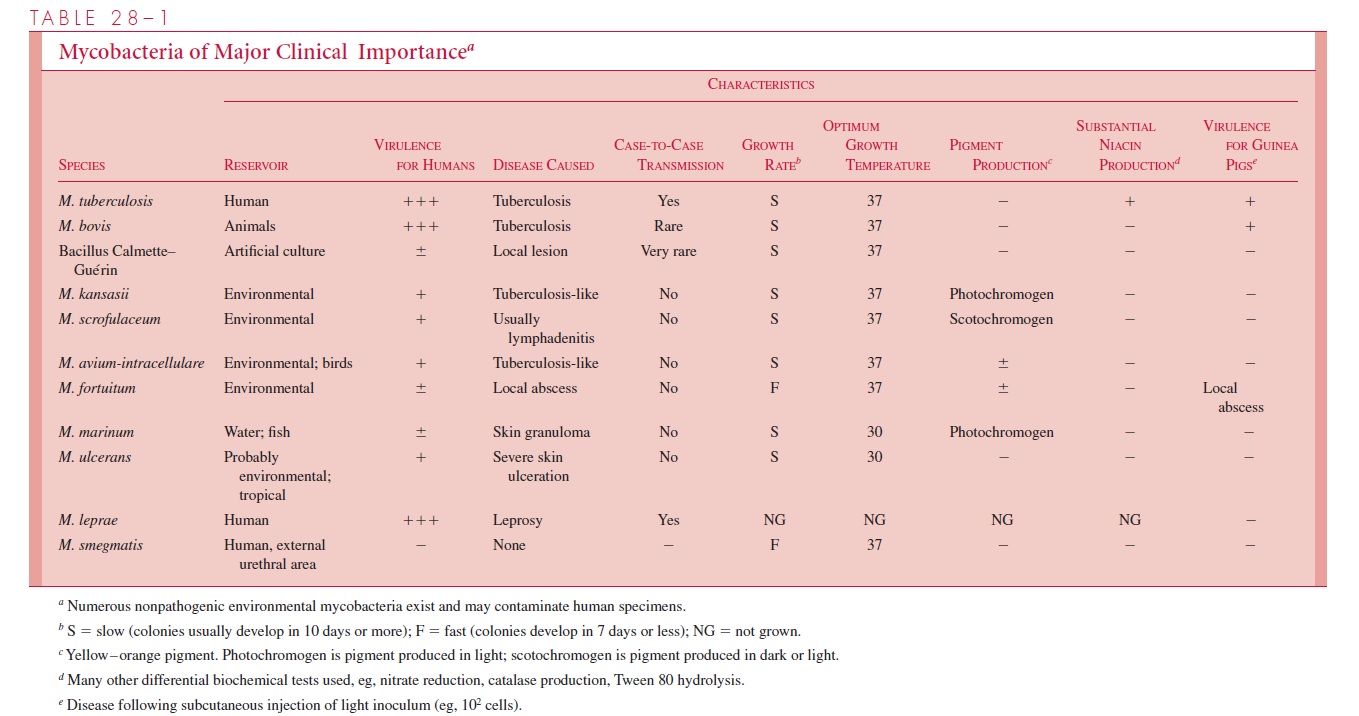
Mycobacteria causing diseases that often resemble tuberculosis are listed in Table 28 – 1. With the exception of M. bovis, they have become relatively more prominent as the incidence of tuberculosis has declined. All have known or suspected environmental reser-voirs, and all the infections they cause appear to be acquired from these sources. Immunocompromised individuals or those with chronic pulmonary conditions or malig-nancies are more likely to develop disease. There is no evidence of case-to-case transmis-sion. The organisms grow on the same media as M. tuberculosis but usually more rapidly. Colonies of some species produce yellow or orange pigment in the light (photochro-mogenic), and some in the light and dark (scotochromogenic). Species are distinguished by these characteristics and by biochemical reactions. Environmental mycobacteria that cause tuberculosis-like infections are usually more resistant than M. tuberculosis to some of the antimicrobics used in the treatment of mycobacterial diseases, and susceptibility testing is often needed as a guide to therapy.
Mycobacterium kansasii
Mycobacterium kansasii is a photochromogenic mycobacterium that usually formsyellow-pigmented colonies after about 2 weeks of incubation in the presence of light. In the United States, infection is most common in Illinois, Oklahoma, and Texas and tends to affect urban residents; it is uncommon in the Southeast. There is no evidence of case-to-case transmission, but the reservoir has yet to be identified. It causes about 3% of mycobacterial disease in the United States.
M. kansasii infections resemble tuberculosis and tend to be slowly progressive withouttreatment. Cavitary pulmonary disease, cervical lymphadenitis, and skin infections are most common, but disseminated infections also occur. They are an important cause of disease in patients with HIV infection and CD4+ T lymphocyte counts of less than 200 cells/ L; clinical features closely resemble tuberculosis in patients with AIDS. Hypersensitivity to proteins of M. kansasii develops and cross-reacts almost completely with that caused by tuberculosis. Positive PPD tests may thus result from clinical or subclinical M. kansasii infection. Prolonged combined chemotherapy with isoniazid, rifampin, and ethambutol is usually effective.
Mycobacterium avium – Intracellulare Complex
Mycobacterium avium – intracellulare complex is a group of related acid-fast organismsthat grow only slightly faster than M. tuberculosis and can be divided into a number of serotypes. Among them are organisms that cause tuberculosis in birds (and sometimes swine) but rarely lead to disease in humans. Others may produce disease in mammals, in-cluding humans, but not in birds. They are found worldwide in soil and water and in in-fected animals. In the United States they are most common in the Southeast, Pacific Coast, and north central regions. They are second only to M. tuberculosis in significance and frequency of the diseases they cause.
The most common infection in humans is cavitary pulmonary disease, often superim-posed on chronic bronchitis and emphysema. Most individuals infected are white men of 50 years of age or more. Cervical lymphadenitis, chronic osteomyelitis, and renal and skin infections also occur. The organisms in this group are substantially more resistant to antituberculous drugs than most other species, and treatment with the three or four agents found to be most active often requires supplementation with surgery. About 20% of cases relapse within 5 years of treatment.
Disseminated M. avium – intracellulare infections, once considered rare, are now the most common systemic bacterial infection in patients with AIDS. They usually develop when the patient’s general clinical condition and CD4+ helper T lymphocyte concentra-tions are declining. Clinically, the patient experiences progressive weight loss and inter-mittent fever, chills, night sweats, and diarrhea. Histologically, granuloma formation is muted, and there are aggregates of foamy macrophages containing numerous intracellular acid-fast bacilli. The diagnosis is most readily made by blood culture, using a variety of specialized cultural techniques. Identification can be rapidly accomplished with the use of specific DNA probes. Response to chemotherapeutic agents is marginal, and the prog-nosis is grave.
Mycobacterium scrofulaceum
Mycobacterium scrofulaceum is an acid-fast scotochromogen that occurs in the environ-ment under moist conditions. It forms yellow colonies in the dark or light within 2 weeks, and it shares several features with the M. avium – intracellulare complex. Mycobacteriumscrofulaceum is now one of the more common causes of granulomatous cervical lym-phadenitis in young children. It derives its name from scrofula, an old descriptive term for tuberculous cervical lymphadenitis. The infection manifests as an indolent enlargement of one or more lymph nodes with little, if any, pain or constitutional signs. It may ulcerate or form a draining sinus to the surface. It does not cause PPD conversion. Treatment usually involves surgical excision.
Related Topics