Chapter: Essential Anesthesia From Science to Practice : Clinical management : Airway management
Mask ventilation - Airway management techniques
Airway management techniques
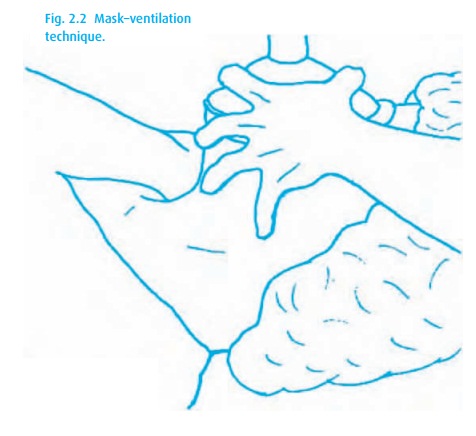
Mask–ventilation
Simple
as it seems, the ability to mask–ventilate a patient is the essential airway management technique that needs to be practised
and learned by every health-care provider. Most important is the patient’s head
position: Do not let the patient’s neck flex and thus potentially occlude the
airway, which makes mask–ventilation difficult to impossible. Proper mask
technique includes the following:
(i) Select an appropriate size mask to fit over the
patient’s nose and mouth and provide an airtight seal without pressure on the
eyes.
(ii) Place the head in sniffing position (occiput
elevated, neck extended) or directly supine, with the neck neutral to slightly
extended.
(iii) Positioning yourself at the patient’s head,
apply the mask to the face with a pincer grip by thumb and index finger of the
left hand. Place the third finger on the mentum and pull the chin upward. The
fourth finger remains on the mandible so as not to compress the soft tissue,
with the pinkie at the angle of the mandible where the jaw can be pushed
forward to open the posterior pharynx (a painful maneuver in an awake patient!)
(Fig. 2.2).
(iv) Then ventilate the patient’s lungs with a self-inflating
bag, Mapleson or anesthesia machine circle system. Keep inflation pressures to
the minimum required to ventilate the lungs, in an effort to prevent inflation
of the stomach.
What to
do when mask–ventilation proves to be difficult:
·
Reposition. Make sure the mandible is being pulled anteriorly.
·
Add a second person to try two-handed mask–ventilation. Use both
hands to hold the mask and pull the jaw anteriorly. The other person compresses
the breathing bag.
·
Use an oral or nasal airway to establish a pathway past the
pharyngeal tissue and tongue. This is not advisable in the awake patient (he
would retch) nor under light anesthesia (he might develop a tight laryngospasm,
which would make matters worse). A nasal trumpet can be inserted after lubrication
with a local anesthetic jelly, even if the patient is awake.
·
If the patient has a beard, try placing an occlusive dressing (with
a hole for the mouth) over the beard, or apply Vaseline to the mask.
·
The edentulous patient usually does better with his false teeth in
place. If the patient is comatose, an oral airway may help, or stuff the cheeks
with gauze to provide enough shape for the mask to seal properly. Just be sure
to remove all material from the mouth when the patient is ready to resume
spontaneous breathing – material left behind has been aspirated and has caused
acute airway obstruction and death!
Related Topics