Chapter: Essential Anesthesia From Science to Practice : Clinical management : Airway management
Laryngeal mask airway - Airway management techniques
Laryngeal mask airway
Developed
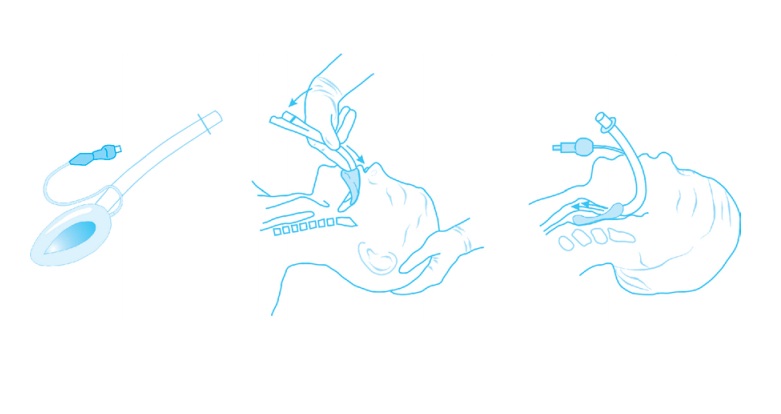
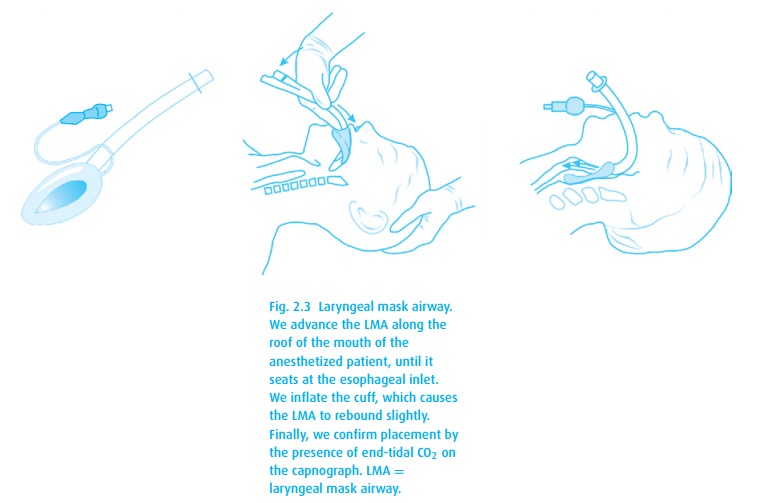
in the 1980s, the laryngeal mask airway (LMA; Fig. 2.3)
has supplanted tracheal intubation for many general anesthetics. The device is
basically the progeny of a facemask mated with an endotracheal tube, allowing
positioning of the mask just above the glottic opening. While we have available
a version intended to protect the airway from gastric aspiration (LMA
Proseal®), none can guarantee it. The major advantages of the LMA over tracheal
intubation are the lower level of skill required for placement, decreased
airway trauma (especially of the vocal cords), and reduced stimulation such
that lightly anesthetized, sponta-neously breathing patients can tolerate the
device. Also, the properly positioned LMA places the laryngeal inlet in clear
view for a fiberoptic scope, making tra-cheal intubation through the device a
popular technique in the management of the difficult airway.
To place
the LMA, we induce anesthesia without paralysis, then
1.
place the patient’s head in the sniffing position;
2.
stabilize the occiput and slightly extend the neck with the right
hand, allowing the jaw to fall open;
3.
press the deflated LMA against the hard palate with the gloved
index fin-ger, and gently advance it until encountering the resistance of the
upper esophageal sphincter.
There
are many variations to this technique, including the popular initial inser-tion
upside-down, then rotation in the posterior pharynx (not recommended by the
manufacturer). When difficulty arises, try moving to the front of the patient,
placing the right hand on the top of the LMA and using the index finger to coax
the tip of the LMA down toward the laryngeal inlet. Any restriction to the
mouth opening makes that impossible. When correctly positioned, the cuff comes
to sit at the base of the hypopharynx. The vocal cords (and many times the
esopha-gus) will come into view within the LMA bowl. Thus, this airway does not
protect against aspiration. While it can be used during controlled ventilation,
we risk gastric distension if inflation pressure exceeds 20 cm H2O.
We
remove the LMA from the awake patient after suctioning above the cuff and then
deflating it. Because the LMA is less stimulating than an endotracheal tube,
and unlikely to produce laryngospasm upon its removal, in the spontaneously
breathing patient the LMA can be removed in the PACU by nursing staff, thereby
reducing anesthetic wake-up time in the OR and improving OR throughput.
Related Topics