Chapter: Essential Anesthesia From Science to Practice : Clinical management : Airway management
Examination of the airway - Anesthesia Clinical management
Examination of the airway
Direct
laryngoscopy (see below) requires neck flexibility, a mouth that can open
widely, and no excessive pharyngeal tissue or a large tongue to get in the way.
These features cannot be measured directly, but the following steps help us to
assess problems that might arise during laryngoscopy:
·
Assess mouth opening: inter-incisor distance should exceed 4 cm in
an adult.
·
Determine the mentum–hyoid (>4 cm) or thyromental (>7 cm) distance: shorter distances suggest an
anterior or very cephalad larynx, which would be difficult to visualize by
laryngoscopy.
·
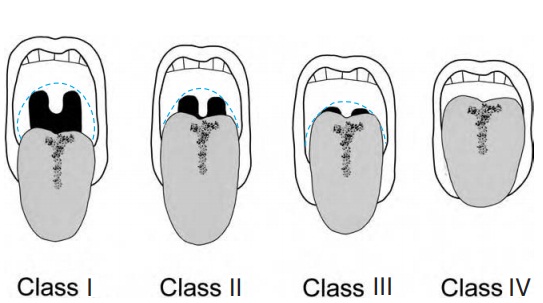
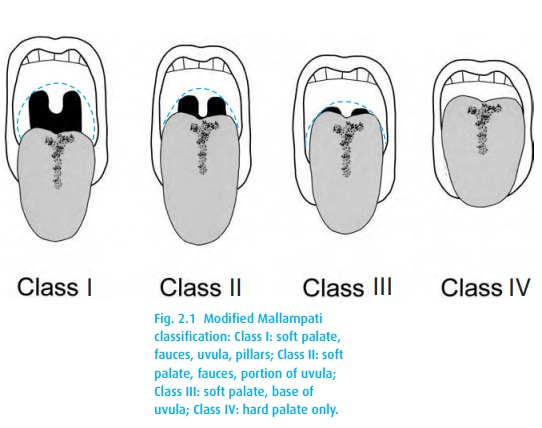
Investigate the posterior pharynx (modified Mallampati
Classification) by hav-ing the sitting patient fully extend his neck, maximally
open his mouth, and stick out his tongue with or without phonation. Figure 2.1shows how we classify the visible structures.
·
Determine the ability to move lower in front of the upper incisors,
which is a good sign.
·
Evaluate neck mobility: full extension through full flexion should
exceed 90°. Patients who require further evaluation include:
o those with rheumatoid arthritis and/or Down’s
syndrome: the transverse ligament that secures the odontoid can become lax,
introducing the poten-tial for cervical cord trauma with direct laryngoscopy;
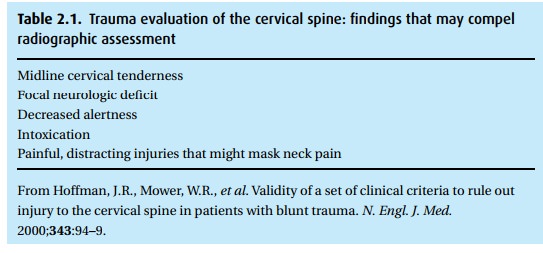
o trauma patients who may have damaged their
cervical spine (Table 2.1).
· Finally, patients with a history of difficult intubation and any obvious airway pathology (vocal cord tumor, neck radiation scar, congenital malformation, etc.)
·
should be further investigated. Patients with a history of snoring
and/or morbid obesity also cause us concern.
Related Topics