Chapter: Essential Anesthesia From Science to Practice : Clinical management : Airway management
Airway management plan
Airway management plan
For many
operative procedures requiring general anesthesia, any of these tech-niques
(mask, LMA, ETT) may be appropriate, but there are times to prefer one
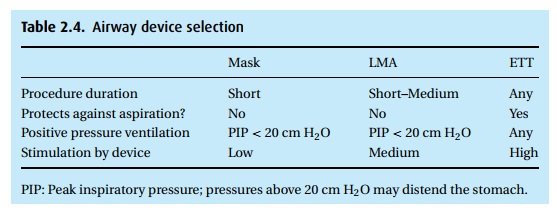
We take into account the planned procedure and the patient’s status
(Table 2.4). An emergency laparoscopic
appendectomy should probably be performed with an ETT because of the high risk
of aspiration (full stomach and increased intra-abdominal pressure from
laparoscopy), while a professional singer undergoing a minor elective procedure
might be better served with a mask or LMA.
A word
about the patient with a potentially unstable cervical spine. Many times,
trauma patients arrive from the Emergency Department without a “cleared”
cer-vical spine. Though radiographs can identify fractures and displacement,
they fail to reveal torn or damaged ligaments, all pointing to instability of
the cervical spine. If the patient is intoxicated or comatose and thus can give
neither a useful history nor report cervical pain, we are in a quandary: the
trauma patient’s full stomach suggests the need for rapid sequence intubation
to minimize the risk of aspiration, while direct laryngoscopy may traumatize
the spinal cord. The options become these:
·
An airway technique One that does not require neck movement, such
asintubating through an LMA, using a lighted stylet, or retrograde intubation.
In skilled hands, these techniques may be performed with relative speed. A
lengthy process increases the likelihood of aspiration.
·
wake fiberoptic intubation May be difficult in an intoxicated,
uncoopera-tive patient, and may take too long in the patient with multiple
traumatic injuries.
·
Blind nasal intubation Again, skilled hands dramatically increase the
likeli-hood of success, but this technique is contra-indicated in the presence
of a base-of-skull fracture, e.g., with “raccoon eyes” or with CSF dripping
from the nose, as the endotracheal tube can enter the brain.
·
Direct laryngoscopy with in-line stabilization A second person stabilizes theneck (without
pulling on the head) in an effort to minimize neck extension. While probably
inadequate in the patient with known cervical spine injury, this technique
might be used for the patient with a low likelihood of trauma whose “clearance”
was limited only by intoxication.
·
Awake tracheostomy Far more invasive than the other techniques, we
reservethis primarily for patients with upper airway trauma that will prevent
other intubation techniques.
Regardless
of the technique selected, the physician administering any general anesthetic
must be prepared for a failure of that plan and ready to institute an
alternative airway management technique. Finally, extra pairs of skilled hands
are always useful. Call for help early
when things are not going as planned!
Related Topics