Chapter: Essential Anesthesia From Science to Practice : Clinical management : Airway management
Awake fiberoptic intubation - Airway management techniques
Awake fiberoptic intubation
Sometimes
an indirect visualization technique becomes necessary, either dur-ing airway
rescue, or when a pre-operative examination suggests a likelihood of
In such cases, perhaps the most definitive technique is to secure
the airway while the patient is still awake and breathing spontaneously. Awake
fiberoptic intubation requires topical anesthesia for the patient’s com-fort,
as well as to blunt the gag reflex that would prevent successful intubation of
the trachea. All too frequently, secretions will smear the optics of the scope:
an anti-sialogogue can be helpful.
Several
nerves are involved in the sensation of the upper airway (Fig. 2.8). It is not much of a mnemonic, but try to
remember a variant to TGIF (Thank God it’s Friday) namely TGIR: “Thank God it’s recurrent.” It’s lame, but perhaps just lame
enough to be memorable! All but the first of these make up the gag reflex.
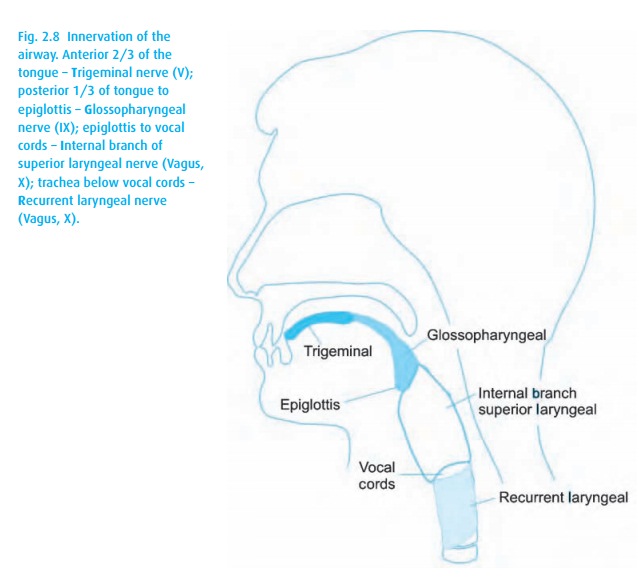
We
anesthetize the posterior tongue and oro/nasopharynx by either spraying 4%
lidocaine or having the patient gargle viscous lidocaine. Glossopharyngeal
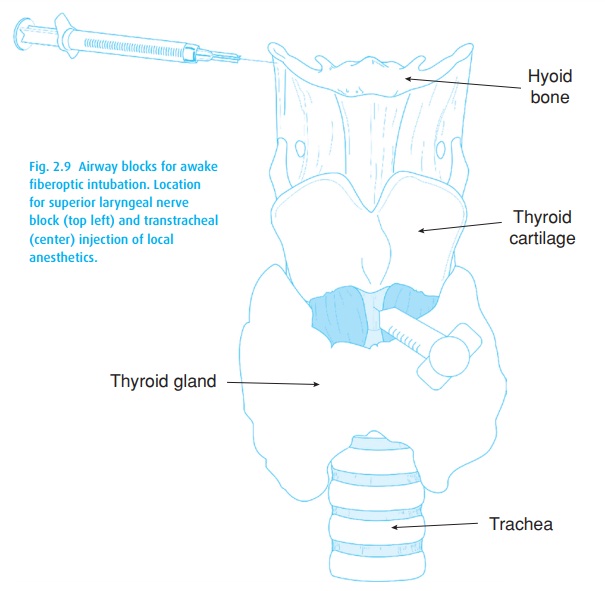
blocks also work well. We block the superior laryngeal nerves by injecting 1%
lidocaine close to where the nerves penetrate the thyrohyoid membrane (Fig. 2.9).
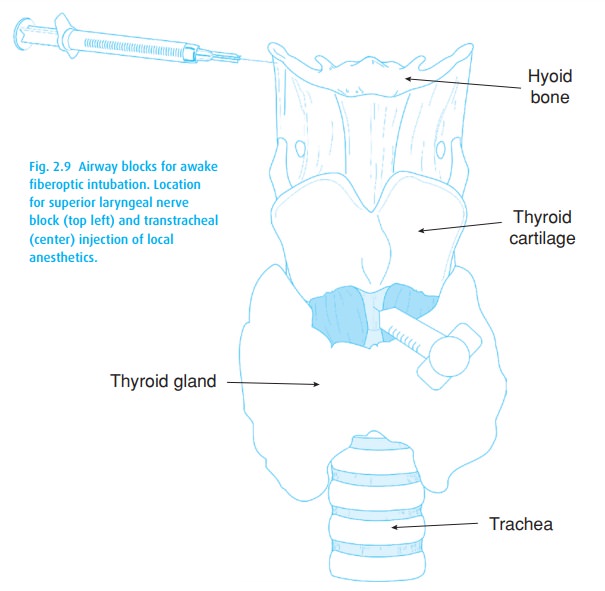
The transtracheal block is accomplished by injecting 2–4% lidocaine directly into the tracheal lumen through the cricothyroid membrane (after confirming needle location
by easily aspirating air). Be sure to point the needle toward the carina. You
are very close to the vocal cords, which you do not want to damage with a
needle pointed cephalad!
This
technique is better tolerated with sedation, though the risk : benefit of
potential airway compromise and aspiration – more likely with a numbed larynx –
must always be taken into account.
Related Topics