Chapter: Modern Medical Toxicology: Chemical Poisons: Heavy Metals
Magnesium - Chemical Poisons
Magnesium
·
Magnesium is a white mineral element
which is an important component of the human body present in soft tissue,
muscle, bone, and body fluids. Normal magnesium level of serum varies from 1.5 to
2.5 mEq/L. Magnesium found in normal urine ranges from 2 to 4 mEq/L (1 to 6
mmol/L). A 24-hour urine specimen is important to assess magnesium excretion
accurately due to circadian variation.
·
Magnesium is ingested via water and several types of food.
Deficiency is rare, except in diarrhoea and malabsorp-tion states and is
characterised by neuromuscular hyperexcit-ability (sometimes accompanied by
behavioural disturbances), absence of other electrolyte or toxic causes,
failure to respond to IV calcium, and response to IV magnesium. Manifestations
include muscular weakness, tremors, ataxia, vertigo, focal or generalised
tonic-clonic seizures, irritability, depression or psychotic behaviour and
decreased respirations.
·
Magnesium salts are used in pharmacotherapeutics as antacids
(magnesium trisilicate, magnesium carbonate, magne-sium hydroxide, i.e. milk of
magnesia), laxatives (magnesium citrate, magnesium hydroxide or milk of
magnesia, magnesium oxide, magnesium phosphate, and magnesium sulfate),
anti-pyretic (magnesium salicylate), anticonvulsant (magnesium sulfate), and
for correction of electrolyte disturbances as well as in dialysis solutions
(magnesium chloride).
·
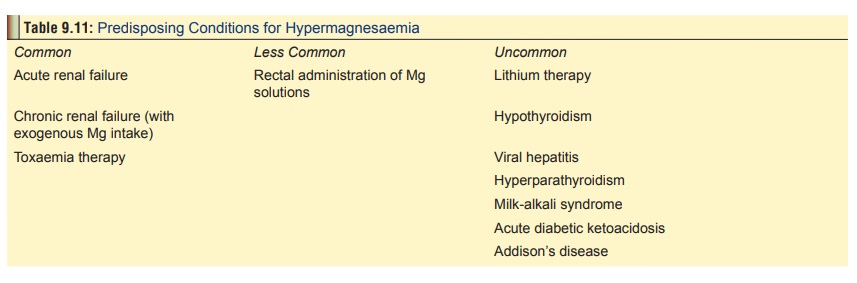
Magnesium salts rarely cause poisoning since the kidneys
normally excrete the magnesium ion with sufficient rapidity to prevent its
accumulation. However, hypermagnesaemia can occur in the presence of renal
failure and certain other predisposing conditions (Table 9.11). In such situations, it is dangerous to administer
repeated doses of magnesium salts unless careful monitoring is done of deep
tendon reflexes, bowel motility, renal function, and serum calcium and
magne-sium levels.
Mode of Action
·
Hypermagnesaemia impairs
neuromuscular junction transmis-sion by decreasing acetylcholine release from
the presynaptic membrane, by diminishing the depolarising action of
acetylcho-line at the postsynaptic junction, and by impairing postsynaptic
junction sensitivity to acetylcholine.
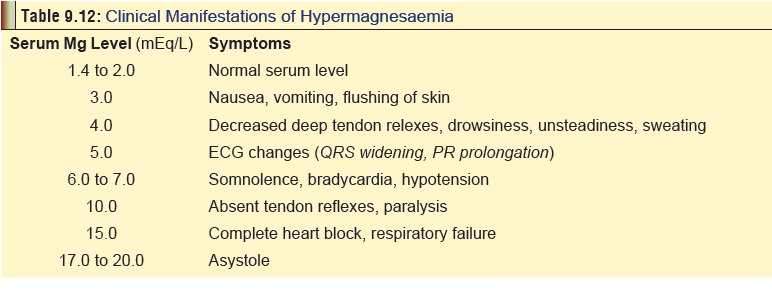
Clinical Features
·
These have been correlated with the
serum magnesium level and mentioned in Table
9.12.
· Paediatric poisoning—Infants often manifest sleepiness, limp muscle tone, and poor suck reflex. Impaired renal func-tion is the most common cause of hypermagnesaemia in the paediatric population. High dose (>48 grams) tocolytic magnesium sulfate therapy was reported to be associated with increased perinatal mortality among foetuses and neonates weighing 700–1249 grams in one case-control study.
Treatmen
·
Discontinue magnesium intake.
·
Eliminate magnesium by enema if it
is in the bowel.
·
Calcium gluconate is the antidote
for hypermagnesaemia. 10% solution is administered IV (10 to 20 ml in adults,
100 mg/kg in children upto a maximum of 1 gram, slowly, over 5 to 10 minutes,
with ECG monitoring). Alternatively calcium chloride 10% can be given IV (0.2
to 0.5 ml/kg/dose up to 10 ml/dose over 5 to 10 minutes). Repeat dose as
needed. Monitor ECG and stop infusion if heart rate begins to decrease.
·
Furosemide (40 mg in adults, 1 mg/kg
in children) along with replacement of urine volume by 0.9% saline, may be
useful as an altenative therapy.
·
Haemodialysis or exchange
transfusion.
Related Topics