Chapter: Modern Medical Toxicology: Chemical Poisons: Heavy Metals
Barium - Chemical Poisons
Barium
Important
derivatives include barium sulfate, sulfide, chloride, and carbonate.
Uses
·
Rat poison—barium carbonate, hydroxide, or chloride.
·
Depilatory—barium sulfide.
·
Gastrointestinal x-ray—barium sulfate (the “barium meal”).
·
Golf balls—barium sulfate (along with calcium carbonate, zinc sulfide, castor
oil, and fish oils).
·
All water or acid soluble barium salts are highly toxic. The
most commonly involved in poisoning (accidental or intentional) are the
following: barium carbonate (a white powder), barium fluoride, barium sulfide,
barium oxide (a white to yellowish powder), barium chloride, barium acetate,
and barium sulfate (water-insoluble, white or yellowish, odourless, tasteless,
fine, heavy orthorhombic powder or crystalline solid).
Usual Fatal Dose
·
Barium carbonate—60 to
70 mg/kg
·
Barium chloride—12 to 20
mg/kg
·
It has been reported that the LD50
for barium ingestion is 1 gram.
Mode of Action
·
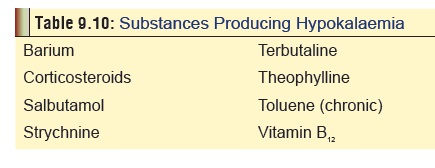
Hypokalaemia (Table 9.10), and neuromuscular blockade: The rapid onset of the
marked hypokalaemia so charac-teristic of barium intoxication is due to
sequestering of potassium by muscle cells. Barium clogs the exit channel for
potassium ions in skeletal muscle cells.
·
Barium stimulates striated, smooth,
and cardiac muscle resulting in violent peristalsis, arterial hypertension and
arrhythmias.
Clinical Features
·
GIT—Salivation,
vomiting, abdominal pain, diarrhoea.
·
CNS—Mydriasis,
paraesthesias, depressed tendon reflexes,headache, confusion, convulsions.
·
CVS—Hypertension,
cardiac arrhythmias (prematureventricular complexes, ventricular tachycardia,
bradycardia and ventricular fibrillation asystole/fibrillation.
·
LMS—Myoclonus,
myalgia, cramps, dysarthria, flaccidquadriplegia.
·
RS—Pulmonary
oedema, respiratory failure.
·
Hypokalaemia, metabolic and
respiratory acidosis, and renal failure are commonly reported. In fact,
quadriplegia is usually the result of severe hypokalaemia.
·
Oral or rectal barium sulfate
administration may cause constipation, impaction, obstruction, cramping,
diarrhoea, and perforation of the bowel. Appendicitis, bowel perfo-ration,
peritonitis and proctitis have been reported after oral or rectal barium
sulfate use in radiologic procedures. ECG abnormalities have also been
reported. Aspiration of barium sulfate may cause pneumonitis, granuloma
forma-tion, severe dyspnoea, and hypoxaemia. Barium sulfate is almost insoluble
and lacks the severe toxicity characteristic of ingestion of other salts.
·
Allergic reactions (including
anaphylaxis) can occur following barium sulfate administration for radiologic
purposes.
Diagnosis
·
X-ray of abdomen.
·
Blood barium level.
Treatment
·
Gastric decontamination (emesis,
lavage). For lavage, 5 to 10 grams sodium sulfate can be added to the solution.
·
Monitor cardiac rhythm and serum
potassium. Cardiac ![]() arrhythmias usually respond to potassium
administration.
arrhythmias usually respond to potassium
administration.
If not, consider lignocaine, amiodarone, or procainamide.
·
IV fluids (liberally, to flush out
barium by diuresis). Administer 0.45% NaCl in D5W, and a diuretic such as
intravenous furosemide (1 mg/kg to a maximum of 40 mg/ dose) to obtain a urine
flow of 3 to 6 ml/kg/hr. Saline and furosemide forced diuresis has been
reported to enhance barium elimination. If initial hydration is necessary,
admin-ister 0.45% saline to which sodium bicarbonate has been added to bring to
isotonic 80 mEq/L at 20 to 30 ml/kg/hr for the first few hours. 30 grams
magnesium sulfate through a nasogastric tube (250 mg/kg for children). It
precipitates the compound ingested into insoluble barium sulfate. In the past
intrave-nous magnesium sulfate was recommended. This should be avoided because
renal injury may result due to intrarenal precipitation of barium sulfate.
·
Treat hypokalaemia with potassium
infusions (up to 250 mEq administered over 24 hours has been effective).
·
Haemodialysis.
·
Mild to moderate allergic reactions
to barium sulfate administration can be managed with antihistamines, with or
without inhaled beta agonists, corticosteroids or adrenaline. Treatment of
severe anaphylaxis necessitates oxygen supplementation, aggressive airway
management, adrenaline, ECG monitoring, and IV fluids.
Autopsy Features
·
Haemorrhagic gastritis and
duodenitis.
·
Pulmonary oedema.
Forensic Issues
·
Most cases are accidental, usually
the result of mistaken iden- tity, when a soluble barium salt is administered
for a “barium meal” instead of the insoluble barium sulfate. Barium salts are
sometimes also mistakenly ingested in place of Epsom salt, Glauber’s salt, or
even common salt. Inhalation of a “barium meal” can produce granulomas in the
lungs.
A
few cases of mass poisonings have been reported, the most remakable being Pa Ping an endemic form of periodic
paralysis which occurred in the early 1940s in the Szechuan province of China.
This was due to massive contamination of table salt by barium chloride.
Related Topics