Chapter: Basic & Clinical Pharmacology : Adrenoceptor Agonists & Sympathomimetic Drugs
Indirect-Acting Sympathomimetics
Indirect-Acting Sympathomimetics
As
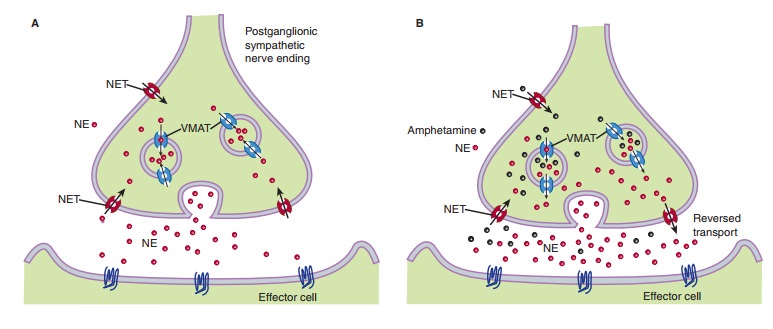
noted previously, indirect-acting sympathomimetics can have one of two
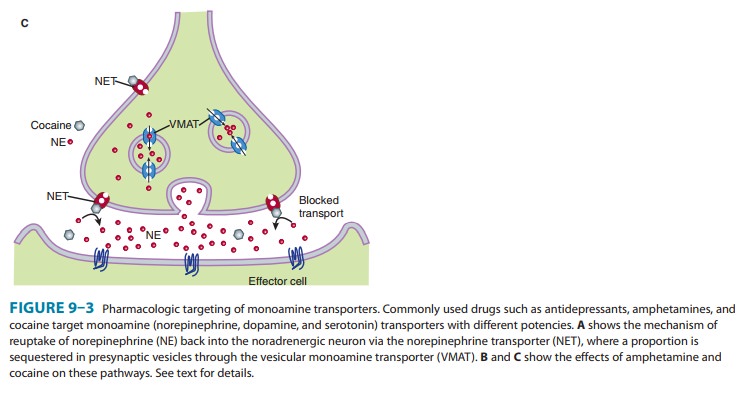
different mechanisms (Figure 9–3). First, they may enter the sympathetic nerve
ending and displace stored cate-cholamine transmitter. Such drugs have been
called amphetamine-like or “displacers.” Second, they may inhibit the reuptake
of released transmitter by interfering with the action of the norepi-nephrine
transporter, NET
A. Amphetamine-Like
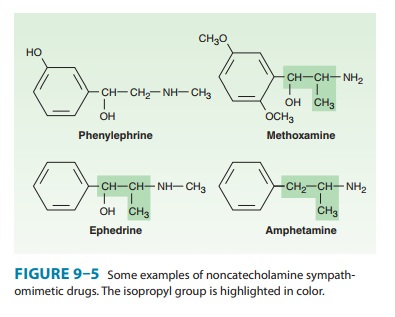
Amphetamine is a racemic mixture of
phenylisopropylamine(Figure 9–5) that is important chiefly because of its use
and misuse as a central nervous system stimulant . Pharmacokinetically, it is
similar to ephedrine; however, amphet-amine even more readily enters the central
nervous system, where it has marked stimulant effects on mood and alertness and
a depressant effect on appetite. Its D-isomer is more potent than the L-isomer.
Amphetamine’s actions are mediated through the release of norepinephrine and,
to some extent, dopamine.
Methamphetamine (N-methylamphetamine)
is very similar toamphetamine with an even higher ratio of central to
peripheral actions. Phenmetrazine is
a variant phenylisopropylamine with amphetamine-like effects. It has been
promoted as an anorexiant and is also a popular drug of abuse. Methylphenidate is an amphetamine
variant whose major pharmacologic effects and abuse potential are similar to
those of amphetamine. Methylphenidate may be effective in some children with
attention deficit hyperactivity disorder (see Therapeutic Uses of
Sympathomimetic Drugs). Modafinil is
a psychostimulant that differs from amphetamine in structure, neurochemical
profile, and behavioral effects. Its mechanism of action is not fully known. It
inhibits both norepinephrine and dopamine transporters, and it increases
synaptic concentrations not only of norepinephrine and dopamine, but also of
serotonin and glutamate, while decreasing GABA levels. It is used primarily to
improve wakefulness in nar-colepsy and some other conditions. It is often
associated with increases in blood pressure and heart rate, though these are
usually mild (see Therapeutic Uses of Sympathomimetic Drugs).
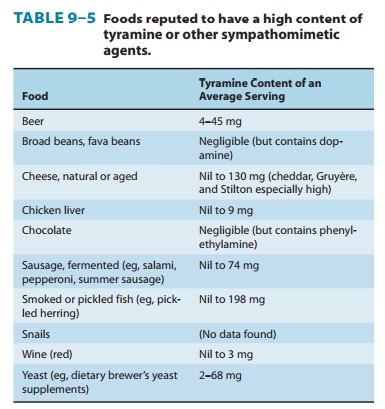
Tyramine (see Figure 6–5) is a normal by product of
tyrosinemetabolism in the body and can be produced in high concentra-tions in
protein-rich foods by decarboxylation of tyrosine during fermentation (Table
9–5). It is readily metabolized by MAO in the liver and is normally inactive
when taken orally because of a very high first-pass effect, ie, low
bioavailability. If administered paren-terally, it has an indirect
sympathomimetic action caused by the release of stored catecholamines.
Consequently, tyramine’s spec-trum of action is similar to that of
norepinephrine. In patients treated with MAO inhibitors—particularly inhibitors
of the MAO-A isoform—this effect of tyramine may be greatly intensi-fied,
leading to marked increases in blood pressure. This occurs because of increased
bioavailability of tyramine and increased neuronal stores of catecholamines.
Patients taking MAO inhibi-tors must be very careful to avoid
tyramine-containing foods. There are differences in the effects of various MAO
inhibitors on tyramine bioavailability, and isoform-specific or reversible
enzyme antagonists may be safer.
B. Catecholamine Reuptake Inhibitors
Many
inhibitors of the amine transporters for norepinephrine, dop-amine, and
serotonin are used clinically. Although specificity is not absolute, some are
highly selective for one of the transporters. Many antidepressants,
particularly the older tricyclic antidepressants, can inhibit norepinephrine
and serotonin reuptake to different degrees. This may lead to orthostatic
tachycardia as a side effect. Some anti-depressants of this class, particularly
imipramine, can induce ortho-static hypotension presumably by their
clonidine-like effect or by blocking α1 receptors, but the mechanism remains unclear.
Atomoxetine is a selective inhibitor of the
norepinephrinereuptake transporter. Its actions, therefore, are mediated by
poten-tiation of norepinephrine levels in noradrenergic synapses. It is used in
the treatment of attention deficit disorders . Atomoxetine has surprisingly
little cardiovascular effect because it has a clonidine-like effect in the
central nervous system to decrease sympathetic outflow while at the same time
potentiating the effects of norepinephrine in the periphery. However, it may
increase blood pressure in some patients. Norepinephrine reuptake is particularly
important in the heart, especially during sympa-thetic stimulation, and this
explains why atomoxetine and other norepinephrine reuptake inhibitors
frequently cause orthostatic tachycardia. Reboxetine
has similar characteristics as atomox-etine. Sibutramine is a serotonin and norepinephrine reuptake inhibitor
and was initially approved by the FDA as an appetite suppressant for long-term
treatment of obesity. It has been taken off the market in the United States and
several other countries because it has been associated with a small increase in
cardiovascu-lar events including strokes in patients with a history of
cardiovas-cular disease, which outweighed the benefits gained by modest weight
reduction. Duloxetine is a widely
used antidepressant with balanced serotonin and norepinephrine reuptake
inhibitory effects . Increased cardiovascular risk has not been reported with
duloxetine. Duloxetine and milnacipran,
another serotonin and norepinephrine transporter blocker, are approved for the
treatment of pain in fibromyalgia .
Cocaine is a local anesthetic with a peripheral
sympathomi-metic action that results from inhibition of transmitter reuptake at
noradrenergic synapses (Figure 9-3). It readily enters the central nervous
system and produces an amphetamine-like psychological effect that is shorter
lasting and more intense than amphetamine. The major action of cocaine in the
central nervous system is to inhibit dopamine reuptake into neurons in the
“pleasure centers” of the brain. These properties and the fact that a rapid
onset of action can be obtained when smoked, snorted into the nose, or
injected, has made cocaine a heavily abused drug . It is interesting that
dopamine-transporter knockout mice still self-administer cocaine, suggesting
that cocaine may have addi-tional pharmacologic targets.
Dopamine Agonists
Levodopa, which is converted to dopamine in the body,
and dop-amine agonists with central
actions are of considerable value inthe treatment of Parkinson’s disease and
prolactinemia. Fenoldopam is a D1-receptor
agonist that selectively leads toperipheral vasodilation in some vascular beds.
The primary indica-tion for fenoldopam is in the intravenous treatment of
severe hypertension .
Related Topics