Chapter: Medical Physiology: The Body Fluid Compartments: Extracellular and Intracellular Fluids; Interstitial Fluid and Edema
Clinical Abnormalities of Fluid Volume Regulation: Hyponatremia and Hypernatremia
Clinical Abnormalities of Fluid Volume Regulation: Hyponatremia and Hypernatremia
The primary measurement that is readily available to the clinician for evaluating a patient’s fluid status is the plasma sodium concentration. Plasma osmolarity is not routinely measured, but because sodium and its associ-ated anions (mainly chloride) account for more than 90 per cent of the solute in the extracellular fluid, plasma sodium concentration is a reasonable indicator of plasma osmolarity under many conditions. When plasma sodium concentration is reduced more than a few milliequivalents below normal (about 142 mEq/L), a person is said to have hyponatremia. When plasma sodium concentration is elevated above normal, a person is said to have hypernatremia.
Causes of Hyponatremia: Excess Water or Loss of Sodium
Decreased plasma sodium concentration can result from loss of sodium chloride from the extracellular fluid or addition of excess water to the extracellular fluid (Table 25–4). A primary loss of sodium chloride usually results in hypo-osmotic dehydration and is associated with decreased extracellular fluid volume. Conditions that can cause hyponatremia owing to loss of sodium chloride include diarrhea and vomiting.Overuse ofdiuretics that inhibit the ability of the kidneys to con-serve sodium and certain types of sodium-wasting kidney diseases can also cause modest degrees of hyponatremia. Finally, Addison’s disease, which results from decreased secretion of the hormone aldosterone, impairs the ability of the kidneys to reabsorb sodium and can cause a modest degree of hyponatremia.
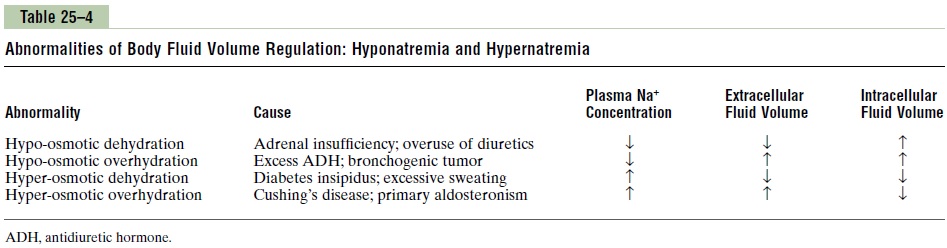
Hyponatremia can also be associated with excess water retention, which dilutes the sodium in the extra-cellular fluid, a condition that is referred to as hypo-osmotic overhydration. For example, excessive secretion of antidiuretic hormone, which causes the kidney tubules to reabsorb more water, can lead to hypona-tremia and overhydration.
Causes of Hypernatremia: Water Loss or Excess Sodium
Increased plasma sodium concentration, which also causes increased osmolarity, can be due to either loss of water from the extracellular fluid, which concentrates the sodium ions, or excess sodium in the extracellular fluid. When there is primary loss of water from the extracellular fluid, this results in hyperosmotic dehydra-tion. This condition can occur from an inability tosecrete antidiuretic hormone, which is needed for the kidneys to conserve water. As a result of lack of anti-diuretic hormone, the kidneys excrete large amounts of dilute urine (a disorder referred to as diabetesinsipidus), causing dehydration and increased concen-tration of sodium chloride in the extracellular fluid. In certain types of renal diseases, the kidneys cannot respond to antidiuretic hormone, also causing a type of nephrogenic diabetes insipidus.A more common causeof hypernatremia associated with decreased extracellu-lar fluid volume is dehydration caused by water intake that is less than water loss, as can occur with sweating during prolonged, heavy exercise.
Hypernatremia can also occur as a result of excessive sodium chloride added to the extracellular fluid. This often results in hyperosmotic overhydration because excess extracellular sodium chloride is usually associ-ated with at least some degree of water retention by the kidneys as well. For example, excessive secretion of thesodium-retaining hormone aldosterone can cause a milddegree of hypernatremia and overhydration. The reason that the hypernatremia is not more severe is that increased aldosterone secretion causes the kidneys to reabsorb greater amounts of water as well as sodium.
Thus, in analyzing abnormalities of plasma sodium concentration and deciding on proper therapy, one should first determine whether the abnormality is caused by a primary loss or gain of sodium or a primary loss or gain of water.
Related Topics