Chapter: The Massage Connection ANATOMY AND PHYSIOLOGY : Respiratory System
Breathing Patterns, Respiratory Volumes, and Capacities
BREATHING PATTERNS, RESPIRATORY VOLUMES, AND CAPACITIES
Breathing Patterns
The number of breaths taken every minute is known as the respiratory rate; a normal adult has a respi-ratory rate of about 12–18 breaths per minute. Children breathe about 18–20 breaths per minute. The normal rate of inspiration to expiration is 2:1. Eup-nea is the term for normal, quiet breathing. A patternof breathing in which the breathing is shallow, with the chest moving outward, is known as costalbreathing. This movement is a result of the contrac-tion and relaxation of the intercostals muscles that move the ribs. In diaphragmatic breathing, the di-aphragm moves up and down, pushing the abdomi-nal contents outwards.
Respiratory Volumes and Capacities
The respiratory rate and the volume of air moving in and out of the lungs can be easily recorded using the spirometer, or respirometer. The recording ob- tained is thespirogram (see Figure 10.11). An up-ward deflection is produced in the recording when a person breathes in through the mouthpiece of the spirometer. Expiration is recorded as a downward de-flection. The height of deflection reflects the volume breathed; the horizontal axis reflects time.
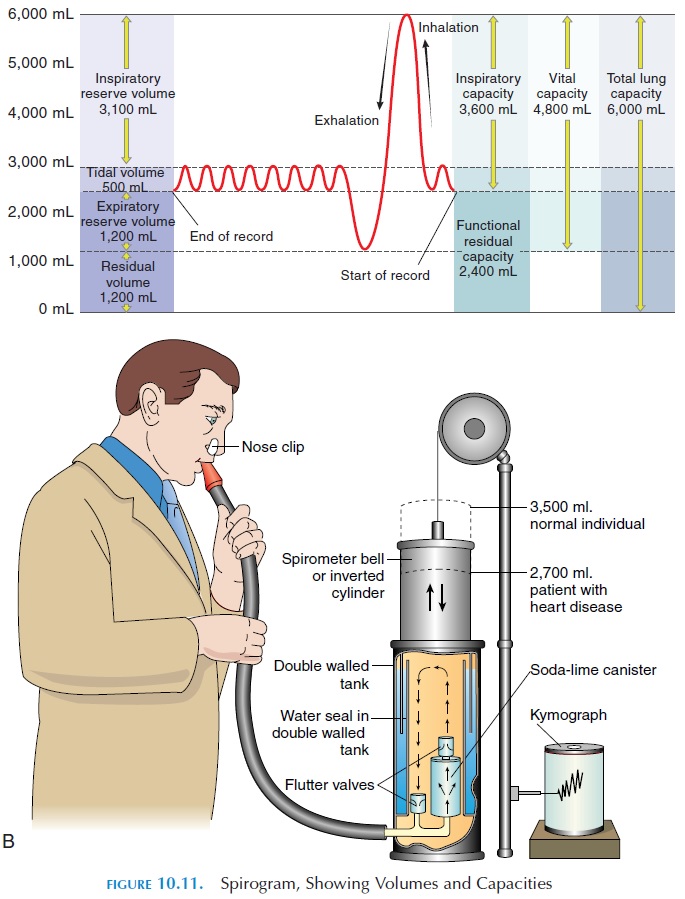
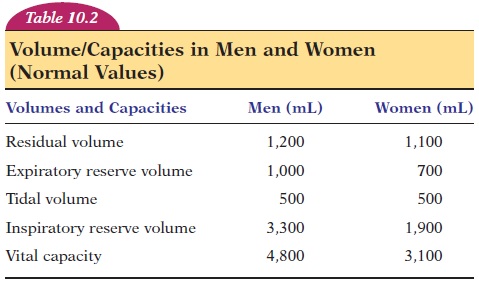
At rest, breathing quietly, an adult takes in about 500 mL (30.5 in3) of air. This is known as tidal vol-ume (see Table 10.2). Thus, the volume of airbreathed in and out every minute during quiet respi-ration is equal to respiratory rate tidal volume and is about 6.0 liters (1.6 gal) per minute. This volume is known as the respiratory minute volume.
The total volume of air that can be accommodated in the respiratory system is known as the total lungcapacity. This volume averages about 6 liters (1.6gal) in men and 4.2 liters (1.1 gal) in women. Of total lung capacity, the volume of air that a person can breathe in after a normal expiration is much more than the tidal volume. This volume, known as the in-spiratory capacity, includes the inspiratory reserve volume and tidal volume (the approximate values inmen and women are given in Table 10.2). The volume of air that a person can breathe out after a normal ex-piration is known as the expiratory reserve volume.
Even when a person breathes out as forcefully as pos-sible, there is some air remaining in the lungs. This volume of air is known as the residual volume. The residual volume and the expiratory reserve volume together make up the functional residual capacity.Vital capacity is the volume of air that a person canmaximally breathe out after a maximal inspiration. Sometimes, the volume of air a person can forcefully breathe out in the first second is measured. This vol-ume is known as the forced expiratory volume inone second (FEV1), or timed vital capacity. Nor-mally, more than 80% of the total volume expired is expelled in the first second. FEV1 is reduced in con-ditions where obstruction to the airway is present. FEV1 is a useful measurement for monitoring the day-to-day response to drugs, dosage required, and the progress of obstructive diseases in individuals. A small device known as the peak flow meter is often given to patients to track of their forced expiratory volume.
To monitor gas exchange, blood samples may be analyzed to determine the concentration of dissolved gases.
The volumes and capacities, as seen in Table 10.2 differ between men and women. Some volumes also vary with the age and height of the individual. People living in high altitudes and those who have led an ac-tive lifestyle since childhood tend to have larger vital capacities.
The vital capacity of an individual does not matter, what is important is the volume of air that actually reaches the exchange surface—the alveoli. This air, known asalveolar ventilation, is equal to 4.2 liters (1.1 gal) per minute. Because the air that occupies the space in the conducting passages (nasal cavity to the terminal bronchiole) are not involved in gas ex-change, this volume of air is referred to as deadspace air. More specifically, this volume of air isknown as anatomic dead space because this wasted air is a result of the anatomic structure; it occupies about 150 mL (9.2 in3).
Other than the anatomic dead space, some air taken into the lungs may be wasted if the alveoli that they enter do not have a blood supply. Here, although air reaches the exchange surface, there is no blood circulation for gas exchange to take place. The vol-ume of such wasted air is known as physiologicdead space. In normal individuals, this dead space is low. However, in individuals with such conditions as fibrosis of the lungs, the dead space is large and gas exchange is inadequate.
Related Topics