Chapter: Basic & Clinical Pharmacology : Beta-Lactam & OtherCell Wall- & Membrane-Active Antibiotics
Beta-Lactamase Inhibitors (Clavulanic Acid, Sulbactam, & Tazobactam) - Beta Lactam Drugs
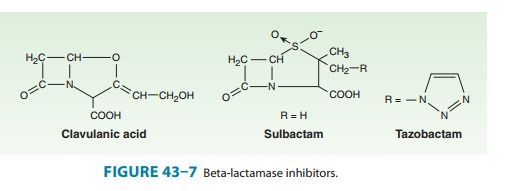
BETA-LACTAMASE INHIBITORS
(CLAVULANIC ACID, SULBACTAM, & TAZOBACTAM)
These substances
resemble β-lactam
molecules (Figure 43–7), but they have very weak antibacterial action. They are
potent inhibitors of many but not all bacterial β lactamases and can protect hydrolyz-able
penicillins from inactivation by these enzymes. Beta-lactamase
inhibitors are most active against Ambler class A β lactamases (plasmid-encoded
transposable element [TEM] β lactamases in particular), such as those produced
by staphylococci, H influenzae, N gonorrhoeae, salmonella, shigella, E coli,
and K pneumoniae. They are not good inhibitors of class C β lactamases, which
typically are chromosomally encoded and inducible, produced by Enterobacter sp,
Citrobacter sp, S marcescens, and P aeruginosa, but they do inhibit chromosomal
β lactamases of B fragilis and M catarrhalis.
The three inhibitors differ
slightly with respect to pharmacol-ogy, stability, potency, and activity, but
these differences usually are of little therapeutic significance.
Beta-lactamase inhibitors are available only in fixed combinations with
specific penicillins. The antibacterial spectrum of the combination is
determined by the companion penicillin, not the β-lactamase inhibitor. (The fixed combinations
available in the USA are listed in Preparations Available.) An inhibitor
extends the spectrum of a penicillin pro-vided that the inactivity of the
penicillin is due to destruction by
lactamase
and that the inhibitor is active against the β lactamase that is produced. Thus,
ampicillin-sulbactam is active against β-lactamase-producingS aureusandH influenzaebut not againstserratia, which produces a β lactamase
that is not inhibited by sulbactam. Similarly, if a strain of P aeruginosa is resistant to
piperacillin, it is also resistant to piperacillin-tazobactam because
tazobactam does not inhibit the chromosomal β lactamase pro-duced by P aeruginosa.
The indications for
penicillin-β-lactamase
inhibitor combina-tions are empirical therapy for infections caused by a wide
range of potential pathogens in both immunocompromised and immu-nocompetent
patients and treatment of mixed aerobic and anaero-bic infections, such as
intra-abdominal infections. Doses are the same as those used for the single
agents except that the recom-mended dosage of piperacillin in the
piperacillin-tazobactam combination is 3–4 g every 6 hours. Adjustments for
renal insuf-ficiency are made based on the penicillin component.
Related Topics