Chapter: Clinical Anesthesiology: Anesthetic Management: Maternal & Fetal Physiology & Anesthesia
Anesthesia for Physiological Changes During Pregnancy
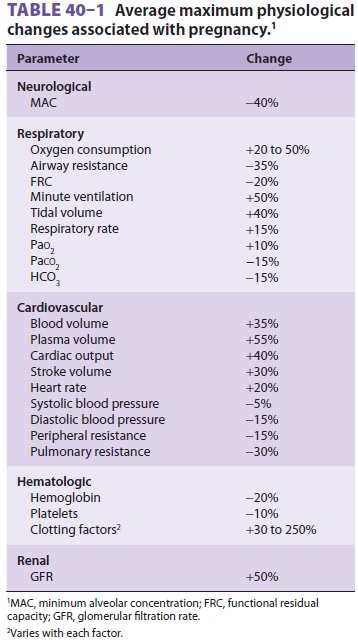
PHYSIOLOGICAL CHANGES DURING PREGNANCY
Pregnancy affects most organ systems (Table
40–1). Many of these physiological changes appear
to be adaptive and useful to the mother in tolerating the stresses of
pregnancy, labor, and delivery. Other changes lack obvious benefits but
nonetheless require special consideration in caring for the parturient.
Central Nervous System Effects
The minimum alveolar concentration (MAC) progressively decreases during
pregnancy-at term, by as much as 40%—for all general anes-thetic agents; MAC
returns to normal by the third day after delivery. Changes in maternal hormonal
and endogenous opioid levels have been impli-cated. Progesterone, which is
sedating when given in pharmacological doses, increases up to 20 times normal
at term and is at least partly responsible for this
observation. A surge in β-endorphin
levels during labor and delivery also likely plays a major role.Pregnant
patients also display enhanced sen-sitivity to local anesthetics during
regionalanesthesia and analgesia, and neural blockade
occurs at reduced concentrations of local anesthet-ics. The term minimum local
analgesic concentra-tion (MLAC) is used in obstetric anesthesia to compare the
relative potencies of local anesthetics and the effects of additives; MLAC is
defined as the local analgesic concentration leading to satisfac-tory analgesia
in 50% of patients (EC50). Local anesthetic dose requirements during epidural
anes-thesia may be reduced as much as 30%, a phenom-enon that appears to be
hormonally mediated but may also be
related to engorgement of the epiduralvenous
plexus. Obstruction of the inferior vena cava by the enlarging uterus distendsthe
epidural venous plexus and increases epidural blood volume. The latter has
three major effects: (1) decreased spinal cerebrospinal
fluid volume, (2) decreased potential volume of the epidural space, and (3)
increased epidural (space) pressure. The first two effects enhance the cephalad
spread of local anesthetic solutions during spinal and epi-dural anesthesia,
respectively, whereas the last may complicate identification of the epidural
space . Bearing down during labor further accentuates all these effects.
Positive (rather than the usual negative) epidural pressures have been recorded
in parturients. Engorgement of the epi-dural veins also increases the
likelihood of placing an epidural needle or catheter in a vein, resulting in an
unintentional intravascular injection. It is unclear whether pregnancy lowers
the seizure threshold for local anesthetics.
Respiratory Effects
Oxygen consumption and minute ventilation
pro-gressively increase during pregnancy. Tidal volume and, to a lesser extent,
respiratory rate and inspi-ratory reserve volume also increase. By term, both
oxygen consumption and minute ventilation have increased up to 50%. Paco2 decreases to 28–32 mm Hg; significant respiratory
alkalosis is prevented by a compensatory decrease in plasma bicarbonate
concentration. Hyperventilation may also increase Pao2 slightly. Elevated levels of
2,3-diphosphoglyc-erate offset the effect of hyperventilation on hemo-globin’s
affinity for oxygen . The P50 for hemoglobin increases from 27 to 30 mm Hg; the combination of the
latter with an increase in cardiac output (see section on Cardiovascular
Effects below) enhances oxygen delivery to tissues.
The maternal respiratory pattern changes as
the uterus enlarges. In the third trimester, elevation of the diaphragm is
compensated by an increase in the anteroposterior diameter of the chest;
diaphrag-matic motion, however, is not restricted. Thoracic breathing is
favored over abdominal breathing. Both vital capacity and closing capacity are
minimally affected, but functional residual capacity (FRC) decreases up to 20%
at term; FRC returns to normal within 48 h of delivery. This decrease is
principally due to a reduction in expiratory reserve volume as a result of
larger than normal tidal volumes. Flow– volume loops are unaffected, and airway
resistance decreases. Physiological dead space decreases but intrapulmonary
shunting increases toward term. A chest film may show prominent vascular
markings due to increased pulmonary blood volume and an elevated diaphragm.
Pulmonary vasodilation pre-vents pulmonary pressures from rising.
The combination of decreased FRC and
increased oxygen consumption promotes rapid oxygen desaturation during periods
of apnea. Preoxygenation (denitrogenation) prior to induc-tion of general
anesthesia is therefore mandatory to avoid hypoxemia in pregnant patients.
Closing volume exceeds FRC in some pregnant women when they are supine at term.
Under these condi-tions, atelectasis and hypoxemia readily occur. The decrease
in FRC coupled with the increase in minute ventilation accelerates the uptake
of all inhalational anesthetics. The reduction in dead space narrows the
arterial end-tidal CO 2 gradient.
Capillary engorgement of the respiratory
mucosa during pregnancy predisposes the upper airways to trauma, bleeding, and
obstruction. Gentle laryngos-copy and smaller endotracheal tubes (6–6.5 mm)
should be employed during general anesthesia.
Cardiovascular Effects
Cardiac output and blood volume increase to
meet accelerated maternal and fetal metabolic demands. An increase (55%) in
plasma volume in excess of an increase in red cell mass (45%) produces
dilutional anemia and reduces blood viscosity. Hemoglobin concentration, however,
usually remains greater than 11 g/dL. Moreover, in terms of tissue oxygen
delivery, the reduction in hemoglobin concentration is offset by the increase
in cardiac output and the rightward shift of the hemoglobin dissociation curve
(see the section on Respiratory Effects). A decrease in systemic vascular
resistance by the second trimes-ter decreases both diastolic and, to a lesser
degree, systolic blood pressure. The response to adrenergic agents and
vasoconstrictors is blunted.
At term, blood volume has increased by 1000–1500 mL in most women,
allowing them to easily tolerate the blood loss associated with deliv-ery;
total blood volume reaches 90 mL/kg. Average blood loss during vaginal delivery
is 400–500 mL, compared with 800–1000 mL for a cesarean sec-tion. Blood volume
does not return to normal until 1–2 weeks after delivery.
The increase in cardiac output (40% at term) is due to increases in both
heart rate (20%) and stroke volume (30%). Cardiac chambers enlarge and
myocardial hypertrophy is often noted on echo-cardiography. Pulmonary artery,
central venous, and pulmonary artery wedge pressures remain unchanged. Most of
these effects are observed in the first and, to a lesser extent, the second
trimes-ter. In the third trimester, cardiac output does not appreciably rise,
except during labor. The greatest increases in cardiac output are seen during
labor and immediately after delivery (see the section on Effect of Labor on
Maternal Physiology). Cardiac output often does not return to normal until 2 weeks
after delivery. Decreases in cardiac output can occur in the supine position
after week 20 of pregnancy. Such decreases have been shown to be secondary to
impeded venous return to the heart as the enlarging uterus compresses the
inferior vena cava.
Approximately 5% of women at term develop the supine hypotension
syndrome (aortocavalcompression), which is characterized by
hypoten-sion associated with pallor, sweating, or nausea and vomiting. The
cause of this syndrome appears to be complete or near-complete occlusion of the
inferior vena cava by the gravid uterus. When combined with the hypotensive
effects of regional or general anesthesia, aortocaval compression can readily
pro-duce fetal asphyxia. Turning the patient on her side typically restores
venous return from the lower body and corrects the hypotension in such
instances. This maneuver is most readily accomplished by placing a wedge (>15°) under the right hip.
The gravid uterus also compresses the aorta in most parturients when they are
supine. This latter effect decreases blood flow to the lower extremities and,
more importantly, to the uteroplacental circulation. Uterine contrac-tion
reduces caval compression but exacerbates aor-tic compression.
Chronic partial caval obstruction in the
third trimester predisposes to venous stasis, phlebitis, and edema in the lower
extremities. Moreover, compres-sion of the inferior vena cava below the
diaphragm distends and increases blood flow through the para-vertebral venous
plexus (including the epidural veins), and to a minor degree, the abdominal
wall.
Lastly, elevation of the diaphragm shifts the
heart’s position in the chest, resulting in the appear-ance of an enlarged
heart on a plain chest film and in left axis deviation and T wave changes on
the elec-trocardiogram. Physical examination often reveals a systolic ejection
flow murmur (grade I or II) and exaggerated splitting of the first heart sound
(S1);
a third heart sound (S3) may be audible. A few patients develop small, asymptomatic pericardial
effusion.
Renal & Gastrointestinal Effects
Renal plasma flow and the glomerular filtra-tion rate increase during
pregnancy, and as a result serum creatinine and blood urea nitrogen may
decrease to 0.5–0.6 mg/dL and 8–9 mg/dL, respectively. A decreased renal tubular
threshold for glucose and amino acids is common and often results in mild
glycosuria (1–10 g/d) or proteinuria (<300 mg/d), or both. Plasma osmolality
decreases by 8–10 mOsm/kg.
Gastroesophageal reflux and esophagitis are
common during pregnancy. Gastric motility is reduced, and upward and
anteriordisplacement of the stomach by the uterus promotes incompetenceof the gastroesophageal sphincter. These fac-tors place the parturient
at high risk for regur-
gitation and pulmonary aspiration. However,
neither gastric acidity nor gastric volume changes signifi-cantly during
pregnancy. Opioids and anticholiner-gics reduce lower esophageal sphincter
pressure, may facilitate gastroesophageal reflux, and delay gastric emptying.
Hepatic Effects
Overall hepatic function and blood flow are
unchanged; minor elevations in serum trans-aminases and lactic dehydrogenase
levels may be observed in the third trimester. Mild elevations in serum
alkaline phosphatase are due to its secretion by the placenta. A mild decrease
in serum albu-min is due to an expanded plasma volume, and as a result, colloid
oncotic pressure is reduced. A 25–30% decrease in serum pseudocholinesterase
activity is also present at term but rarely produces significant prolongation
of succinylcholine’s action. The break-down of ester-type local anesthetics is
not apprecia-bly altered. Pseudocholinesterase activity may not return to
normal until up to 6 weeks postpartum. High progesterone levels appear to
inhibit the release of cholecystokinin, resulting in incomplete emptying of the
gallbladder. The latter, together with altered bile acid composition, can
predispose to the forma-tion of cholesterol gallstones during pregnancy.
Hematological Effects
Pregnancy is associated with a
hypercoagulable state that may be beneficial in limiting blood loss at
delivery. Fibrinogen and concentrations of factors VII, VIII, IX, X, and XII
all increase; only factor XI levels may decrease. Accelerated fibrinolysis can
be observed late in the third trimester. In addition to the dilutional anemia
(see the section on Cardiovascular Effects), leukocytosis (up to 21,000/µL) and
a 10% decrease in platelet count may be encountered dur-ing the third trimester. Because of fetal utilization, iron and folate
deficiency anemias readily develop if supplements of these nutrients are not
taken.
Metabolic Effects
Complex metabolic and hormonal changes occur
during pregnancy. Altered carbohydrate, fat, and protein metabolism favors
fetal growth and devel-opment. These changes resemble starvation, because blood
glucose and amino acid levels are low whereas free fatty acids, ketones, and
triglyceride levels are high. Nonetheless, pregnancy is a diabetogenic state;
insulin levels steadily rise during pregnancy. Secretion of human placental
lactogen, also called human chorionic somatomammotropin, by the pla-centa is
probably responsible for the relative insulin resistance associated with
pregnancy. Pancreatic beta cell hyperplasia occurs in response to an increased
demand for insulin secretion.
Secretion of human chorionic gonadotropin and
elevated levels of estrogens promote hypertrophy of the thyroid gland and
increase thyroid-binding globu-lin; although T4 and T3 levels are elevated,
free T4, free T3, and thyrotropin (thyroid-stimulating hormone) remain
normal. Serum calcium levels decrease, but ionized calcium concentration
remains normal.
Musculoskeletal Effects
Elevated levels of relaxin throughout pregnancy help prepare for
delivery by softening the cervix, inhib-iting uterine contractions, and
relaxing the pubic symphysis and pelvic joints. Ligamentous laxity of the spine
increases the risk of back injury. The lat-ter may contribute to the relatively
high incidence of back pain during pregnancy.
Related Topics