Chapter: Modern Medical Toxicology: Neurotoxic Poisons: Stimulants
Amphetamines - Stimulant Neurotoxic Poisons

Amphetamines
The
original amphetamine, racemic beta-phenylisopropylamine was first synthesised
in 1887, and was marketed in 1932 as a nasal decongestant (Benzedrine inhaler). Widespread abuse led to its ban in 1959.
Source
·
Amphetamine belongs to the phenylethylamine
family with a methyl group substitution in the alpha carbon position. Numerous
substitutions of the phenylethylamine struc-ture are possible, resulting in
several amphetamine-like compounds. These compounds have now collectively come
to be known as “amphetamines”, and include ampheta- mine phosphate, amphetamine
sulfate, benzphetamine, chlorphentermine, clobenzorex hydrochloride, dextroam-
phetamine, diethylpropion, mazindol, methamphetamine, 4-methylthioamphetamine,
methylphenidate, pemoline, phendimetrazine, phenmetrazine, and phentermine.
·
Methamphetamine abuse began in the
1950s and reached a peak in the 1970s. It used to be referred to as “speed” or
“go” (Fig 16.1). In the late 1980s,
a pure preparation of methamphetamine hydrochloride made its appearance for the
first time in Hawaii where it was referred to as “batu”. It quickly made its
way across to the United Kingdom, Australia, Western Europe, and USA, where it
became popular by the slang name “ice” (or “glass”) (Fig 16.2). While ice is produced by the ephedrine reduction method
and is very pure, occurring as large translucent crystals, a variant produced
by an oil-based method is called “crystal” (or “crank”), and is a white to
yellow crystal product.
·
Methamphetamine powder can be inhaled,
smoked, ingested,or injected. Ice and crystal are almost always smoked.
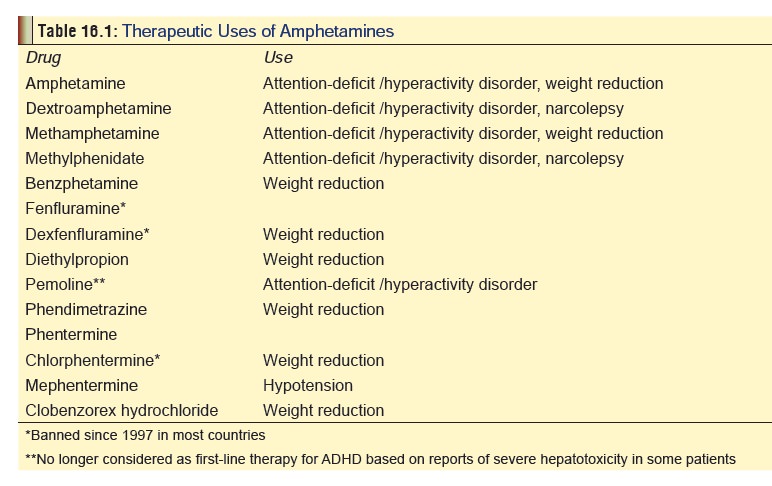
Uses
Some amphetamines have therapeutic uses and are still available as prescription drugs in Western countries (Table 16.1). They are not available in India (except for mephentermine).
Mode of Action
· The major mechanism of acion of amphetamines involves the release of monoamines from storage sites in axon termi-nals, which leads to increased monoamine concentration in the synaptic cleft. The release of dopamine in the nucleus accumbens and related structures is responsible for the reinforcing and mood elevating effects of amphetamines.
·
Methylphenidate has a different mechanism of action. Like
cocaine, it produces CNS action by blocking the dopamine transporters
responsible for the reuptake of dopamine from synapses following its release.
The relatively low abuse potential of orally administered methylphenidate is
due to slow occupation of dopamine transporters in the brain. Also, unlike
cocaine, methylphenidate occupies the transporter sites for a much longer time.
·
The most prominent effects of amphetamines are the
catecholamine effects as a result of stimulation of peripheral alpha and beta
adrenergic receptors. Enhanced concentra- tion of noradrenaline at the locus
coeruleus is responsible for the anorexic and stimulating effects, as well as
to some extent, for the motor-stimulating effects.
·
Cardiovascular effects result from the stimulation of
release of noradrenaline.
Toxicokinetics
·
In general, peak plasma levels are seen in about 30 minutes
after intravenous or intramuscular injection, and about 2 to 3 hours after oral
amphetamine ingestion.
·
Amphetamines are extensively metabolised in the liver, but
much of what is ingested is excreted unchanged in the urine. The excretion
of unchanged amphetamine is dependent on pH, and at urine pH less than 6.6, a
range of 67 to 73% of unchanged drug is excreted in the urine. At urine pH
greater than 6.7, the percent excreted unchanged in the urine is reported to be
17 to 43%.
Clinical Features
Acute Poisoning:
a. CNS:
·
Euphoria
·
Agitation
·
Headache
·
Paranoia
·
Anorexia
·
Hyperthermia: can be
severe, and may result from hypothalamic dysfunction, metabolic and muscle
hyperactivity, or prolonged seizures.
·
Hyperreflexia
·
Choreoathetoid
movements
·
Convulsions: Seizures
are associated with a high mortality rate
·
Intracerebral haemorrhage: Abuse of amphetamine and related
drugs can increase the risk for cerebro-vascular incidents in young adults
·
Coma: If it occurs,
is associated with a high mortality rate.
b. CVS
·
– Tachycardia: Tachycardia is common, however, reflex
bradycardia secondary to hypertension can occur.
·
–– Hypertension:
Hypertension is common following amphetamine use and may result in end organ
damage. Pulmonary hypertension has been associ-ated with methamphetamine use.
Hypotension and cardiovascular collapse may result from severe toxicity, and is
associated with a high fatality rate.
·
–– Arrhythmias.
·
–– Vasospasm.
·
–– Myocardial ischaemia: Infarction can occur (videinfra).
·
–– Cardiomyopathy: Acute and chronic cardiomyo-pathy can
result from hypertension, necrosis, or ischaemia.
c. Sympathetic
Effects:
·
Mydriasis
·
Sweating
·
Tremor
·
Tachypnoea
·
Nausea.
d. Other
Effects:
·
Muscle rigidity.
·
Pulmonary oedema.
·
Ischaemic colitis: More common in
chronic poisoning.
·
Rhabdomyolysis: Develops in patients
with severe agitation, muscular hyperactivity, hyperthermia, or seizures.
·
Metabolic acidosis: This occurs with
severe poisoning, and has even been reported after smoking crystal
methamphetamine.
e. Complications:
·
Psychosis with visual and tactile
hallucinations.
·
Cerebral infarction.
·
Myocardial infarction.
·
Aortic dissection: Several cases of
fatal aortic dissection associated with chronic amphetamine use have been
reported.
·
Ventricular fibrillation.
·
Acute renal failure: Renal failure
may develop secondary to dehydration or rhabdomyolysis in patients with severe
amphetamine poisoning.
·
Use of “ice” is associated with
unique neuropsy- chiatric toxicity. Auditory hallucinations, severe paranoia,
and violent behaviour have been reported.
·
Amphetamines and methamphetamines
can induce spontaneous recurrences of paranoid hallucinatory states known as
“flashbacks”.
Chronic Poisoning:
·
Amphetamines can be taken orally, by
injection, by absorption through nasal and buccal membranes; or by heating,
inhalation of the vapours, and absorption through the pulmonary alveoli.
Inhaled amphetamine is almost immediately absorbed with a rapid onset of
effects. Unlike cocaine, amphetamines can be vapour- ised without much
destruction of the molecule, thus obviating the need for preparing a free-base
form for smoking. As with opiates, the rapid onset of effects from amphetamine
injection or inhalation produces an intensely pleasurable sensation referred to
as “rush”.
·
Manifestations of heavy chronic
amphetamine use:
o Hyperactivity,
hyperexcitability.
o Anorexia,
loss of weight, emaciation: Weight loss is one of the most characteristic
findings with chronic use of amphetamine or its derivatives, and is said to be
the most striking effect in chronic “ice” smoking.
o Vomiting
and diarhoea are common. Ischaemic colitis may occur.
o Stereotyped
behaviour (skin picking, pacing, inter-
o minable
chattering).
o Dyskinesias:
bruxism, tics.
o Paranoid
psychosis, unpredictable violence: The most common symptoms in patients with
meth- amphetamine-induced psychosis were auditory and visual hallucinations,
persecutory delusions, and delusions of reference.
o Heightened
sexual activity initially, follo-wed by impotence and sexual dysfunction.
o Occasionally,
very rapid IV injection of a large dose produces a condition called
“overamped”, charac- terised by inability to speak or move even though
consciousness is fully retained. Blood pressure and temperature are usually
elevated. There may be respiratory distress.
o Deterioration
of social (family problems), physical (slovenly, unkempt appearance),
and economic (loss of job, bankruptcy)
status.
o Adverse
psychological reactions—anxiety reactions, amphetamine psychosis, exhaustion
syndrome, depression and hallucinosis.
·
Medical
complications—cardiomyopathy, vasculitis, pulmonary hypertension, permanent
neurological deficits, HIV infection, hepatitis, endocarditis, osteo- myelitis
and pulmonary abscesses.
·
Obstetric complications (in pregnant
users) — eclampsia, intrauterine growth retardation, prematurity,etc.
Amphetamine use during pregnancy has also been associated with birth defects, increased
risk of cardiac malformations and cleft palate.
·
Intravenous injection abusers may
display skin lesions, such as “tracks”, abscesses, ulcers, cellulitis, or
necro- tising angitis.
·
Withdrawal syndrome: Withdrawal
after prolonged amphetamine abuse may precipitate severe depres- sion and
suicide attempts. Anxiety, abdominal cramps, gastroenteritis, headache,
diaphoresis, leth- argy and dyspnoea may result. Increased appetite is common.
Drug Interactions
·
Sympathomimetics, monoamine oxidase
inhibitors, and tricyclic antidepressants cause potentiation of effects, while
antihistamines cause diminution of effects.
·
Amphetamines may increase
anticonvulsant levels.
Usual Fatal Dose
·
The fatal dose of amphetamines is
highly variable, and while death can occur with as little as 1.5 mg/kg of
metham- phetamine, survival has been recorded with 28 mg/kg. This in fact represents the usual range of
amphetamine’s lethal dose—150 mg to 2 grams. However, because of tolerance,
addicts can tolerate up to 5 grams (single IV dose), or 15 gm/day (smokable
methamphetamine).
·
Lethal blood level is said to be around 0.2 mg per 100 ml,
though addicts can tolerate much higher levels with hardly any toxic effects.
·
Death due to amphetamine toxicity most commonly results from
arrhythmias, hyperthermia, or intracerebral ![]() haemorrhage. In cases of survival, symptoms gradually
resolve as the drug is excreted over a period of 24 to 48 hours.
haemorrhage. In cases of survival, symptoms gradually
resolve as the drug is excreted over a period of 24 to 48 hours.
Diagnosis
· Urine is the specimen of choice.
Levels above 2 mg/100 ml indicate acute toxicity. Methods of analysis include
TLC,
·
RIA, HPLC, and GC-MS. The first three methods often give
false positive results, and hence confirmation of a positive test must always
be done by GC-MS.
· A new method (electron-impact mass
fragmentography) enables detection and even quantitation of methampheta-mine in
hair, nails, sweat, and saliva.
· Hair analysis may provide
documentation of methampheta-mine or other drug exposure for several months or
longer. To obtain hair samples, a new disposable scissors should be used to cut
a very small amount of hair (100 mg total, about the width of a pencil) from
about 10 different places. The hair must be cut as close to the scalp as
possible.
Treatment
Acute Poisoning:
Stabilisation:
·
i IV line, cardiac monitoring.
·
Oxygen.
·
Evaluate blood glucose, BUN, and electrolyte levels.
·
Consider the necessity of a CBC, urinalysis, coagu-lation
profile, chest X-ray, CT scan of head, and lumbar puncture, depending on the
presentation.
·
Measure core temperature.
·
Shock is a poor prognostic sign and needs to be managed
effectively. Consider the need for right-sided heart catheterisation to measure
right-sided filling pressure and cardiac output.
Supportive Measures:
·
Airway management, ventilatory support.
·
Rapid rehydration.
·
Mannitol diuresis promotes myoglobin clearance to prevent
renal failure.
·
Assess psychological and neurological status.
·
v Gastric decontamination (in cases of ingestion) with
appropriate tracheal protection. Activated charcoal is beneficial.
Specific Measures:
·
Anxiety, agitation, and hyperactivity can usually be
controlled with benzodiazepines. Diazepam is the drug of choice, and is
administered in a dose of 10 mg IV at intervals (up to a maximum of 100 mg).
Much larger doses (hundreds of milligrams) may be required to obtain adequate
sedation. Titrate dose to clinical response. Control of agitation is an
important aspect to the treatment of amphetamine overdose, since it often leads
to hyperthermia, a common cause of mortality in amphetamine overdose.
Neuroleptics are generally not preferred since they may aggravate hyperthermia,
convul-sions, and cardiac arrhythmias. Physical restraint is inadvisable, since
resistance against such measures will aggravate rhabdomyolysis and
hyperthermia. Extreme agitation and hallucinations may require the administration
of IV droperidol (up to 0.1 mg/kg). Since haloperidol lowers the seizures
threshold, and is associated with neuroleptic malig-nant syndrome, it is not
advisable.
·
Convulsions can be managed with benzodiaz-epines (IV
diazepam), phenytoin, or barbiturates. Refractory cases may require
curarisation.
·
Hyperthermia should be tackled aggressively with hypothermic
blankets, ice baths, and dantrolene infu-sions. Large IV doses of
benzodiazepines can help.
·
Refractory cases must be subjected to neuromuscular paralysis
and mechanical ventilation.
·
Tachycardia can be managed with beta blockers (atenolol).
Labetolol which has combined alpha and beta blocking effects, may be preferable
if tachycardia is associated with hypertension. Sedation with intra-venous
benzodiazepines (diazepam 5 to 10 mg IV repeated every 5 to 10 minutes as
needed) is usually sufficient for treating hypertension. A short acting,
titratable agent such as sodium nitroprusside should be considered if
unresponsive to benzodiazepines.
·
For ventricular arrhythmias: Lignocaine and amiodarone are
generally first line agents for stable monomorphic ventricular tachycardia.
Sotalol is a good alternative. Amiodarone and sotalol should be used with
caution if the QT interval is prolonged, or if torsades de pointes is involved
in the overdose.
·
Unstable rhythms require cardioversion. Atropine may be used
when severe bradycardia is present, and PVCs are thought to represent an escape
complex.
·
For rhabdomyolysis: Early aggressive fluid replacement is
the mainstay of therapy, and may help prevent renal insufficiency. Diuretics
such as mannitol or furosemide may be needed to maintain urine output. Urinary
alkalinisation is not routinely recommended.
·
Diazepam and chlorpromazine have been effective in treating
amphetamine-induced chorea.
·
Although peritoneal dialysis and haemodialysis have been
demonstrated to enhance elimination of amphetamine, the clinical efficacy of
these procedures in human overdose has not been proven and they are rarely if
ever clinically indicated. Acidification of urine enhances amphetamine
excretion, but may precipitate acute renal failure in patients with
myoglobinuria and is therefore contraindicated.
Chronic Poisoning:
·
Most casual users of amphetamines do not need treat-ment.
Those with moderately severe dependence can be treated on an outpatient basis
without using drugs.
·
Strategies range from residential and ambulatory
detoxi-fication to day treatment, multistep activities, and case It is
preferable to provide a structured and manualised cognitive behavioural
treatment, making use of a combination of group and individual counselling.
·
A wide variety of pharmacological agents have been tried as
adjuncts to (or major elements in) the treatment of amphetamine dependence.
These include drugs such as imipramine and fluoxetine, but results have been
disappointing.
Related Topics