Chapter: Modern Medical Toxicology: Neurotoxic Poisons: Stimulants
Cocaine: Clinical Features - Stimulant Neurotoxic Poisons
Clinical Features
Acute Poisoning:
Hyperthermia—This results from:
·
Augmentation of heat production due to increased
psychomotor activity.
·
Diminution of heat dissipation due to vasoconstric-tion.
·
Direct pyrogenic effect due to action on thermoreg-ulatory
centres in the hypothalamus.
·
Stimulation of calorigenic activity of liver. Body
temperature often soars to 108 to 112°F, and does not respond to conventional
antipyretics. It is often associated with rhabdomyolysis, seizures, and renal
failure.
CNS
effects—
·
Headache: Three patterns of cocaine-induced headaches have
been identified –
n Pattern 1—Develops within minutes, and lasts for 2 to 48 hours. The
headache is usually occipital or bilateral, with associated throbbing,
photophobia, nausea, and vomiting.
n Pattern 2—Occurs during a cocaine “binge”, (4 to 14 days of abuse, 1
to 3 g/day), with onset after a few days, which increases in severity
progressively. It is mostly frontal, with associ-ated throbbing, nausea, and
sometimes diplopia and dizziness.
n Pattern 3—Occurs 1 to 4 days after the last dose of cocaine, and
worsens over the next 1 week with continued abstinence. It is also frontal,
with associated throbbing, nausea, vomiting, photophobia, and occasionally neck
stiffness.
·
Anxiety, agitation.
·
Hyperactivity, restlessness.
·
Tremor, hyperreflexia
·
Convulsions: Generalised tonic-clonic, partial motor, and
partial complex seizure have all been reported. Seizures may be recurrent and
status epilepticus has been reported, particularly in chil-dren. Sometimes
there is lethargy and decreased level of consciousness which can persist up to
24 hours (“cocaine washed out syndrome”).
·
Cerebrovascular accidents are not uncommon, and include
subarachnoid haemorrhage, intrac-erebral haemorrhage, cerebral infarction,
tran-sient ischaemic attacks, migraine-type headache syndrome, cerebral
vasculitis, and anterior spinal artery syndrome. Infarction of the
brainstem/spinal cord has also occurred.
Psychiatric
effects—
·
Paranoid state with suspiciousness, hypervigilance, anxiety.
·
Stereotypy.
·
Hallucinations.
·
Toxic delirium.
Ophthalmologic
effects—
·
Mydriasis and/or loss of eyebrow and eyelash hair from
smoking crack cocaine may occur.
·
Corneal abrasions/ulcerations due to particulate matter in
smoke (“crack eye”).
·
Central retinal artery occlusion and bilateral blind-ness
due to diffuse vasospasm. Retinal foreign body granuloma may occur with IV
abuse.
CVS
effects—
·
Tachycardia.
·
Systemic arterial hypertension.
·
Coronary artery vasoconstriction
with myocardial ischaemia and infarction.
·
Tachyarrhythmias of all types can
occur, including sinus tachycardia, atrial fibrillation or flutter, other
supraventricular tachycardias, ventricular premature contractions, ventricular
tachycardia, torsades de pointes, and ventricular fibrillation. Sinus tachycardia
is the most common finding. If hypertension is significant, a reflex
bradycardia may occur.
·
Chronic dilated cardiomyopathy has
been reported.
·
Aortic dissection and rupture.
·
Coronary artery dissection.
·
Sudden cardiac death can occur.
Pulmonary
effects—
·
Thermal injuries to the upper airway
leading to epiglottitis, laryngeal injury, and mucosal necrosis have been
reported after smoking “crack” or free base cocaine.
·
Exacerbation of asthma.
·
Noncardiogenic pulmonary oedema.
·
Pneumothorax, pneumomediastinum.
·
Diffuse alveolar haemorrhage.
·
Bronchiolitis obliterans with organising pneumonia.
Musculoskeletal
effects—
·
Rhabdomyolysis with hyperthermia,
massive elevation of creatine phosphokinase, and acute renal failure: Although
the mechanism of cocaine-associated rhabdomyolysis is unclear, it is
postu-lated that it may result from ischaemia due to vasoconstriction, direct
toxicity, hyperpyrexia, and increased muscle activity from agitation or seizure
activity.
GI
effects—
·
Acute mucosal ischaemia.
·
Colitis.
·
Intestinal perforation: It is
postulated that cocaine blocks the reuptake of noradrenaline leading to
mesenteric vasoconstriction and focal tissue ischaemia and perforation.
·
Pneumoperitoneum has been reported
after smoking crack cocaine.
·
Hepatic necrosis (centrilobular,
midzonal, and panlobar) has been reported in overdose.
Renal
effects—
·
Renal failure, usually secondary to myoglobinuria and
rhabdomyolysis, has been reported after intra-venous or intranasal cocaine use.
·
Renal infarction has occurred following intravenous cocaine
use.![]()
·
Uteroplacental effects—
·
Increased incidence of spontaneous abortion, low
birthweight, and abruptio placentae.
·
Neonatal intoxication may also occur. Infants exposed to
cocaine in utero may display tremu-lousness, impaired orientation, increased
startle response, irritability, muscular rigidity, arousal defi-cits, impaired
motor ability, and lower scores on the
·
Brazelton Neonatal Behavioral Assessment Scale (measuring
interactive behaviour and response to environmental stimuli).
·
There are indications that cocaine may be terato-genic.
Miscellaneous
effects—
·
Priapism has been observed after
topical application of cocaine to the glans penis.
·
Severe metabolic acidosis has been
reported due to seizures, agitation, and hypotension.
Drug
combination effects—
Cocaine
is often combined with other drugs such as ethanol and heroin.
--
Concurrent use of cocaine and ethanol produces additive effects on the brain.
It results in the formation of the metabolite, cocaethylene which is more
cardiotoxic, and is associated with enhanced mortality.
--
Combination of cocaine with heroin is referred to as “speed ball” and is reputed to produce a double effect of initial
high “kick” of cocaine, followed by subsequent euphoric “rush” of heroin. “Speed ball” is usually injected.
Chronic Poisoning:
Cocaine
dependence—
·
Cocaine dependence is defined as a cluster of
physi-ological, behavioural, and cognitive symptoms that, taken together,
indicate that the person continues to use cocaine despite significant problems
related to such use.
·
Some cocaine users can use cocaine intermittently without
becoming dependant, though it is not clear how long such intermittent,
nondependant use can continue. Intermittent use consists of episodes or binges
of use, often starting on weekends and paydays, and lasting until the drug
supply is exhausted or toxicity develops.
·
Such binges, during which the drug may be used every 15 to
30 minutes, can last 7 or more ![]() consecutive days (though usually this extends to only 3 or 4
days). When the binge comes to an end, a “cocaine
crash” occurs.
consecutive days (though usually this extends to only 3 or 4
days). When the binge comes to an end, a “cocaine
crash” occurs.
Cocaine
abuse—
Some cocaine abusers develop
problems or adverse effects related to their drug use (i.e. their use is
maladaptive). Examples of such recurrent mala-daptive patterns include use that
leads to multiple legal problems, failure to meet major social, school, or
work-related obligations, and continued use despite social or vocational
difficulties caused by, or aggravated by cocaine use. When one or more such
substance-related problems occur in a 12-month period, the diagnosis of cocaine
abuse is made.
Chronic use of cocaine leads to CNS
dopamine depletion and increases in the number and sensi-tivity of dopamine
receptors. The dysphoric state associated with cocaine withdrawal (vide infra) and craving for cocaine
appears to be a result of the dopamine-depleted condition.
Features of chronic cocaine use: --
Anorexia, emaciation.
--
Mydriasis
-- Agitation, restlessness: A
cocaine-associated agitated delirium
syndrome has been identified,comprising the following in sequence:
hyper-thermia, delirium with agitation, respiratory arrest, and death.
-- Hallucinations, especially
tactile, characterised by a crawling sensation under the skin (“cocainebugs”) with resultant
excoriation, leading toirregular scratches and ulcers (Magnan’s sign).
Perceptual disturbances or pseudo-hallucina-tions involving vision (“snow
lights”, geometric patterns), smell, hearing, and taste have also been
reported.
--
Tremor.
-- Recurrent chest pain. --
Cardiomyopathy
-- Psychiatric changes: Depression,
psychosis, panic disorders, attention deficit disorders, and eating disorders.
-- Decreased libido, impotence,
gynaecomastia, galactorrhoea, amenorrhoea, and sexual dysfunc-tion are common
with chronic cocaine abuse.
--
“Crack hands”: A syndrome of multiple, black-ened, hyperkeratotic lesions
(linear or circular), of the fingers and palms has been described in crack
cocaine smokers. These lesions probably result from the heat of the glass
cocaine pipe.
-- Maternal chronic cocaine use
during preg-nancy has been suggested as a possible factor in Sudden Infant
Death Syndrome. Cocaine readily passes into breast milk and can cause adverse
effects in the nursing infant.
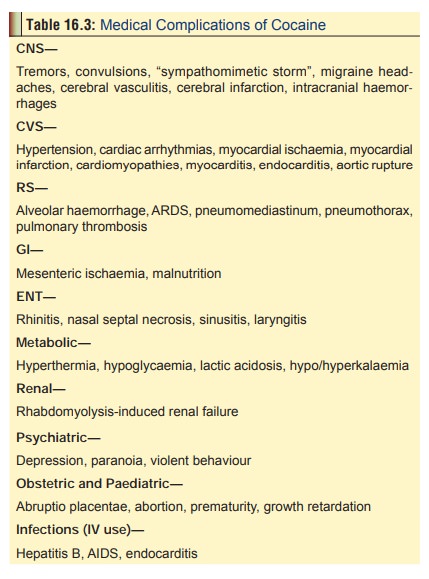
-- Evidence of medical complications (Table 16.3):
»»Extensive bony destruction of the
orbital walls with associated orbital cellulitis may occur in patients with a
history of chronic intranasal cocaine abuse.
»»Intestinal ischaemia following
cocaine ingestion, injection, or crack use has been described.
»»Hepatic damage with elevation of
alanine aminotransferase, aspartate aminotrans-ferase, and alkaline phosphatase
is common.
»»Cocaine withdrawal—Conventionally,
cocaine withdrawal is said to occur in 3 phases:
Phase I—(“Crash”):
-- The total duration of this phase
lasts for anywhere between 9 hours and 4 days, and is subdivided further into
the following stages –
»» Early: Agitation, depression,
anorexia,intense craving for cocaine.
»»Intermediate: Fatigue, tendency to
sleep,decreased craving.
»» Late: Exhaustion, hypersomnia,
hyper-phagia, absence of craving.
Phase II—Normalised sleep, improved mood,followed subsequently by
return of anergia, anhe-donia, anxiety, and increased craving.
Phase III—(“Extinction”): Increased tendency torelapse. The extinction
phase may be prolonged and consists of brief, episodically evoked cravings that
occur months to years after withdrawal.
Usual Fatal Dose
·
About 500 mg (oral)
·
About 100 mg (mucosal contact)
·
Lethal blood level: 0.2
mg/100 ml Chronic users of cocaine can tolerate much higher doses.
Related Topics