Chapter: Clinical Cases in Anesthesia : Malignant Hyperthermia
What are the common causes and associated symptoms of hypoglycemia?
What are
the common causes and associated symptoms of hypoglycemia?
Hypoglycemia is a pathophysiologic state rather
than a disease, and its presence warrants a search for the primary cause.
Hypoglycemia is generally considered the glucose level below which symptoms
appear, but in general, blood glucose determinations below 50 mg/dL are
considered to reflect hypoglycemia. In the conscious patient, hypo-glycemia may
be well compensated with few symptoms or may be associated with diplopia,
blurred vision, sweating, palpitations, or weakness. The clinical presentation
of hypoglycemia is summarized in Table 29.4.
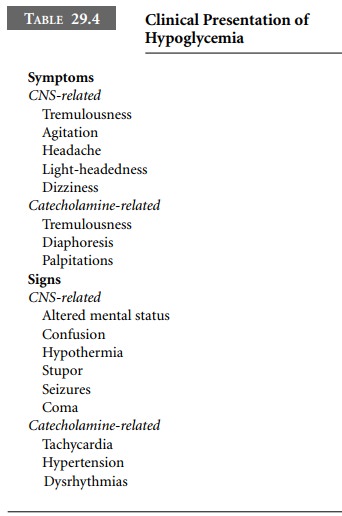
During general anesthesia, the signs and
symptoms of hypoglycemia are nonspecific. They may include sweating and
hypotension or hypertension and tachydysrhythmias. Therefore, serum glucose
assessment is needed to diagnose hypoglycemia during general anesthesia.
Common conditions associated with hypoglycemia
include response to medications (oral hypoglycemic agents, insulin
preparations); ethanol ingestion; tumors of the pancreas or liver; cirrhosis;
hypopituitarism; and adrenal insufficiency. In the perioperative fasting
period, infants, young children, and young adult women may become hypoglycemic
without glucose supplementation. Patients receiving glucose-rich total
parenteral nutrition (TPN) may become hypoglycemic if the infusion is abruptly
discontinued, owing to the insulin levels it contains. Recent recommendations
for patients receiving TPN are to continue the TPN in the operating room and
reduce the infusion rates of other intravenous fluids appro-priately. If TPN
must be discontinued, a solution of 10% dextrose at a rate of approximately 75
mL/hr may be substituted. Glucose levels should be checked to ensure adequate
glucose replacement.
CNS symptoms of hypoglycemia mimic those
com-monly seen in critically ill and sedated patients. Hypoglycemic signs
related to catecholamine release resemble those associated with light anesthesia
and may be misinterpreted. Treatment with β-adrenergic blockers and coexisting autonomic
neuropathy may mask these signs.
Mild episodes of hypoglycemia can be treated
with 5% dextrose boluses and infusions. More significant cases, manifested by
mental status changes, are treated with 50 mL of 50% dextrose, which invariably
causes hyperglycemia. Beneficial responses to glucose administration are both
diagnostic and therapeutic. Continued dextrose adminis-tration may be necessary
following initial treatment.
In the absence of intravenous access,
hypoglycemia can be treated with intramuscular or subcutaneous glucagon.
Diazoxide has been used for prolonged refractory cases such as sulfonylurea
overdose and insulinoma.
Related Topics