Chapter: Medical Surgical Nursing: Assessment and Management of Female Physiologic Processes
Premenstrual Syndrome - Management of Normal and Altered Female Physiologic Processes
PREMENSTRUAL
SYNDROME
Premenstrual syndrome (PMS) is a combination of symptoms that occur before the menses and subside with the onset of men-strual flow (Chart 46-10). The cause is unknown, but serotonin regulation is currently the most plausible theory.
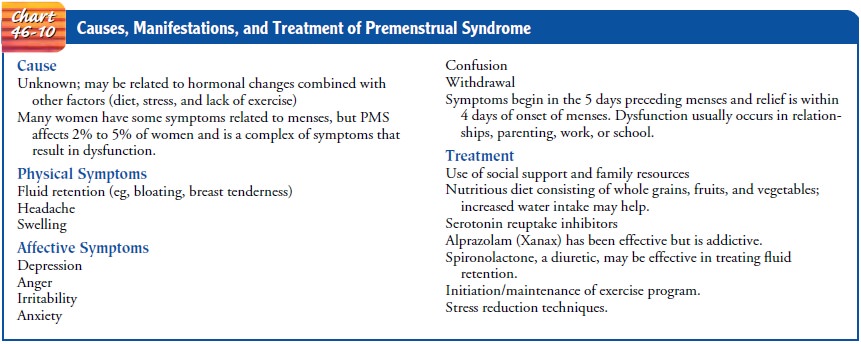
Other hormones may also be involved.
Dietary factors may play a role because car-bohydrates may affect serotonin.
Severe symptoms have been labeled as premenstrual dysphoric disorder (DiCarlo,
Palomba, Tommaselli et al., 2001; Morse, 1999). This severe form of PMS, which
interferes with the woman’s schoolwork, job, or social or family life, is
uncommon.
Clinical Manifestations
Major
symptoms of PMS include headache, fatigue, low back pain, painful breasts, and
a feeling of abdominal fullness. General irritability, mood swings, fear of
losing control, binge eating, and crying spells may also occur. Symptoms vary
widely from one woman to another and from one cycle to the next in the same
per-son. Great variability is found in the degree of symptoms. Many women are
affected to some degree, but few are severely affected. Many women are not
bothered at all, whereas some experience severe and disabling symptoms (Morse,
1999).
A
generally stressful life and problematic relationships may be related to the
intensity of physical symptoms. Some women re-port moderate to severe life
disruption secondary to PMS that negatively affects their interpersonal
relationships. PMS may also be a factor in reduced productivity, work-related
accidents, and absenteeism.
Identifying
the time when these symptoms occur helps in de-termining the diagnosis.
Symptoms recur regularly at the same phase of each menstrual cycle, usually 1
week to a few days before menses, and subside once the menstrual flow starts.
Medical Management
Because
there is no single treatment or known cure for PMS, the woman should chart her
symptoms so she can possibly anticipate and therefore cope with them. Exercise
is encouraged for all pa-tients as noncontrolled studies have shown a benefit.
Many prac-titioners advise women to avoid caffeine, high-fat foods, and refined
sugars, but there is little research to demonstrate the effi-cacy of dietary
changes. Alternative therapies that women have used include vitamins B and E,
magnesium, and oil of evening primrose capsules. No studies have evaluated the
effectiveness of these therapies.
PHARMACOLOGIC THERAPY
Pharmacologic
remedies include selective serotonin reuptake in-hibitors (eg, fluoxetine
[Prozac, Sarafem]), gonadotropin-releasing hormone agonists, prostaglandin
inhibitors (eg, ibuprofen and naproxen [Anaprox]), and antianxiety agents. Some
clinicians prescribe analgesic agents, diuretic medications, and natural and
synthetic progesterones, although the long-term risks of proges-terone use are
unknown. Many women find over-the-counter carbohydrate products useful; they
provide complex carbohy-drates along with vitamins and minerals. Ratios of
serum levels of tryptophan to other amino acids are elevated in patients who
use tryptophan. It may relieve psychological symptoms and food cravings.
Calcium (1,200 mg/day) has been found to be effective, as has magnesium (200 to
400 mg/day).
Nursing Management
The
nurse should establish rapport with the patient and obtain a health history,
noting the time when symptoms began and their nature and intensity. The nurse
then determines whether the onset of symptoms occurs before or shortly after
the menstrual flow begins. Additionally, the nurse can show the patient how to
develop a chart to record the timing and intensity of symptoms. A nutritional
history is also elicited to determine if the diet is high in salt, caffeine, or
alcohol or low in essential nutrients.
The
patient’s goals may include reduction of anxiety (mood swings, crying, binge
eating, fear of losing control), ability to cope with day-to-day stressors and
relationships with family and co-workers, and increased knowledge about PMS
with improved use of control measures.
Positive
coping measures are facilitated. Partners can be ad-vised to assist by offering
support and increased involvement with childcare. The patient can try to plan
her working time to ac-commodate the days she will be less productive because
of PMS. The nurse encourages the patient to use exercise, meditation, imagery,
and creative activities to reduce stress. The nurse also encourages the patient
to take medications as prescribed and provides instructions about the desired
effects of the medications. Enrolling in a PMS group that meets to discuss
problems may help the patient learn that others recognize and understand what
she is experiencing.
If the
patient has severe symptoms of PMS or premenstrual dysphoric disorder, the
nurse assesses her for suicidal, uncontrol-lable, and violent behavior. Any
suggestions of suicidal tenden-cies must be evaluated by psychiatric
consultation immediately. Uncontrollable behavior may lead to violence toward
family members. If abuse of children or other members of the patient’s family
is suspected, reporting protocols are implemented and fol-lowed. Referral is
made for immediate psychiatric or psycholog-ical care and counseling.
Related Topics