Chapter: Ophthalmology: Uveal Tract (Vascular pigmented layer)
Sympathetic Ophthalmia
Sympathetic Ophthalmia
Definition
Specific bilateral inflammation of the uveal
tract due to chronic irritation of one eye, caused by a perforating wound to
the eye or intraocular surgery, pro-duces transferred uveitis in the fellow
eye.
Epidemiology:
Sympathetic ophthalmia is very rare.
Etiology:
Sympathetic uveitis can occur in anotherwise unaffected eyeevenyears after
penetrating injuries or intraocular surgery in the fellow eye, especially where
there was chronic irritation. Tissues in the injured eye (uveal tract, lens,
and retina) act as antigens and provoke an autoimmune dis-order in the
unaffected eye.
Symptoms:
The earliest symptoms include limited range of
accommodationand photophobia. Later there is diminished visual acuity and pain.
Diagnostic considerations:
Clinical symptoms include combined
injections,cells and protein in the anterior chamber and vitreous body,
papillary and ret-inal edema, and granulomatous inflammation of the choroid.
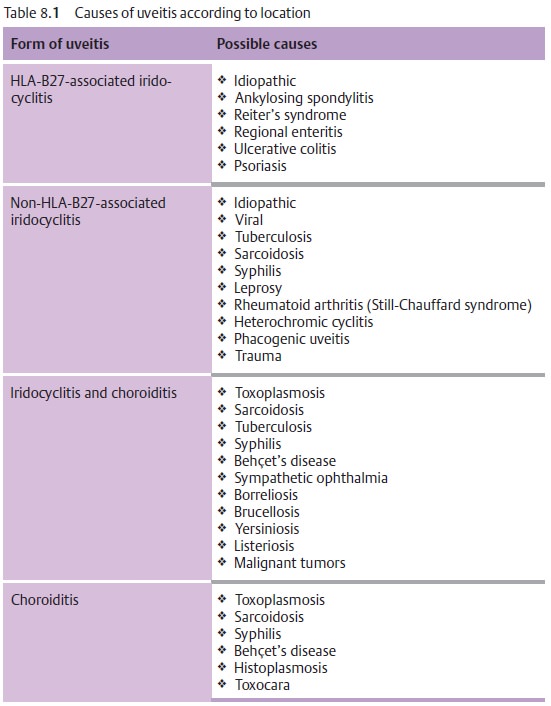
Differential diagnosis:
The disorder should be distinguished from
iridocyclitis and choroiditis from other causes (see Table 8.1).
Treatment:
The injured eye, which is usually blind, must
be enucleated toeliminate the antigen. High-dose topical and systemic steroid
therapy is indi-cated. Concurrent treatment with immunosuppressives
(cyclophosphamide and azathioprine) may be necessary.
Clinical course and complications:
The disorder has a chronic clinical courseand may involve severe
complications of uveitis such as secondary glaucoma,
secondary cataract, retinal detachment, and
shrinkage of the eyeball. Sympa-thetic ophthalmia can lead to blindness in
particularly severe cases.
When the injured eye is blind, prophylactic
enucleation is indicated before the onset of sympathetic ophthalmia in the
fellow eye. An early sign of sympathetic ophthalmia is a limited range of
accommodation with photophobia.
Related Topics