Chapter: Ophthalmology: Uveal Tract (Vascular pigmented layer)
Inflammation in Uveal Tract (Vascular pigmented layer)
Inflammation
Inflammations of the uveal tract are
classified according to the various por-tions of the globe:
❖
Anterior uveitis (iritis).
❖ Intermediate uveitis (cyclitis).
❖ Posterior uveitis (choroiditis). However, some inflammations involve the middle portions of
the uveal tract such as iridocyclitis (inflammation of the iris and ciliary body) or panuveitis (inflammation involving all seg-ments).
Acute Iritis and Iridocyclitis
Epidemiology:
Iritisis the most frequent form of uveitis. It usually occurs
incombination with cyclitis. About three-quarters of all iridocyclitis cases have an acute clinical course.
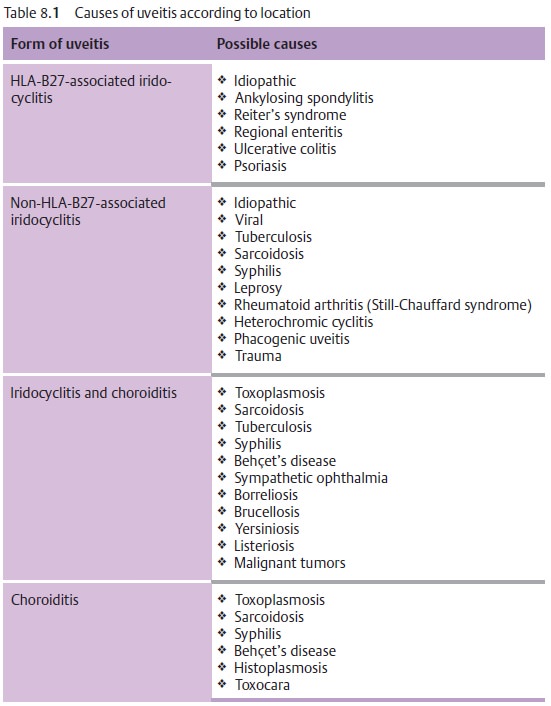
Etiology:
Iridocyclitis is frequently attributable toimmunologic causessuchas allergic or
hyperergic reaction to bacterial toxins. In some rheumatic dis-orders it is
known to be frequently associated with the expression of specific human
leukocyte antigens (HLA) such as HLA-B27. Iridocyclitis can also be a symptom of systemic disease such as
ankylosing spondylitis, Reiter’s syn-drome, sarcoidosis, etc. (Table 8.1). Infections are less frequent and occur sec-ondary to penetrating
trauma or sepsis (bacteria, viruses, mycosis, or para-sites). Phacogenic inflammation, possibly with
glaucoma, can result when the lens becomes involved.
Symptoms:
Patients report dull pain in the eye or
forehead accompanied byimpaired vision, photophobia, and excessive tearing
(epiphora).
In contrast to choroiditis, acute iritis or
iridocyclitis is painful because of the involvement of the ciliary nerves.
Diagnostic considerations:
Typical signs include:
❖Ciliary injection: The episcleral and perilimbal vessels may appear blueand red.
❖Combined injection: The conjunctiva is also affected.
The iris is hyperemic (the iris vessels will be visible in a
light-colored iris).
The structure appears diffuse and reactive miosis is present.
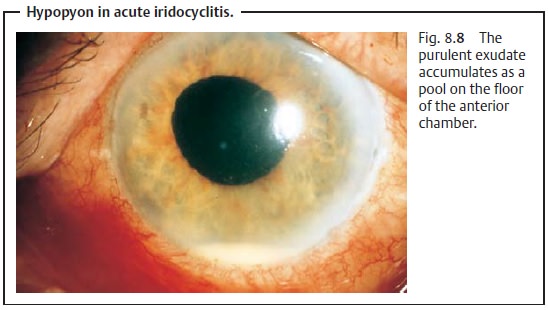
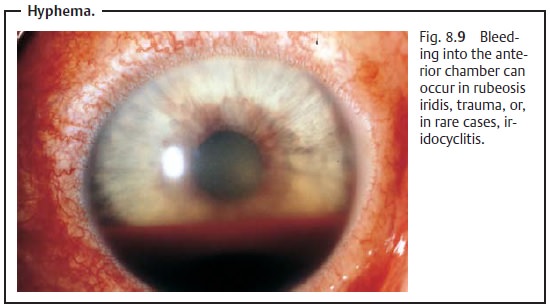
Vision is impaired because of cellular infiltration of the anterior chamber and protein or fibrin accumulation (visible as a Tyndall effect). The precipi-tates accumulate on the posterior surface of the cornea in a triangular con-figuration known as Arlt’s triangle. Exudate accumulation on the floor of the anterior chamber is referred to as hypopyon (Fig. 8.8). Viral infections may be accompanied by bleeding into the anterior chamber (hyphema; Fig. 8.9). Corneal edema can also develop in rare cases.
Corneal edemas and Tyndall effects
(accumulations of protein in the anterior chamber) can be diagnosed when the eye
is illuminated with a lateral beam of light from a focused light or slit lamp.
Differential diagnosis:
See Table 8.2.
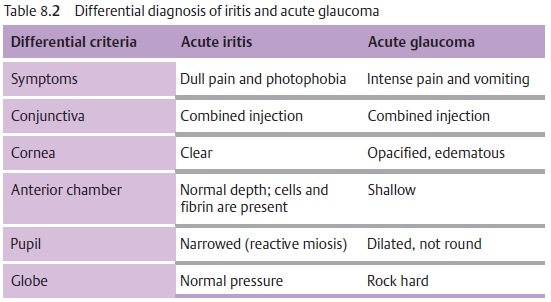
In acute iritis, the depth of the anterior chamber is normal and reactive miosis is present. In contrast, in acute glaucoma the anterior chamber is shallow and the pupil is dilated (Table 8.2).
Complications:
These include:
❖ Secondary open angle glaucoma with an increase in intraocular pressure.
❖ Adhesions between the iris and posterior surface
of the cornea (anterior synechiae).
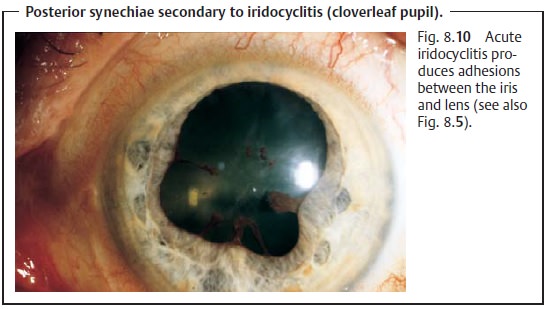
❖
Adhesions between the iris and lens (posterior synechiae; Fig. 8.10).
Treatment:
Topical and, in appropriate cases, systemic antibiotic or
antiviraltherapy is indicated for iridocyclitis due to a pathogen (with a
corneal ulcer, penetrating trauma, or sepsis).
A conjunctival smear, or a blood culture in
septic cases, is obtained to identify the pathogen. Antibiotic therapy should
begin immediately as microbiological identification of the pathogen is not
always successful.
Therapeutic mydriasis in combination with
steroid therapy is indicated to minimize
the risk of synechiae.
Where no pathogen can be identified, high-dose
topical steroid therapy (prednisolone eyedrops every hour in combination with
subconjunctival injections of soluble dexamethasone) is administered. To
minimize the risk of posterior synechiae,
the pupil must be maximally dilated (atropine,scopolamine, cyclopentolate,
and possibly epinephrine and epinephrine eye-drops).
The mydriatic effect of dilating eyedrops may
be reduced in iritis. This may necessitate the use of longer-acting medications
such as atropine, which may have to be applied several times daily.
Occasionally it is possible to break off existing synechiae in this manner, and patches of iris tissue will remain on the
anterior surface of the lens. Second-ary open angle glaucoma is treated by administering beta blockers in
eye-drop form and, in applicable cases, carbonic anhydrase inhibitors
(aceta-zolamide; see Table 10.3).
Prognosis:
Symptoms usually improve within a few days
when proper ther-apy is initiated. The disorder can progress to a chronic
stage.
Chronic Iritis and Iridocyclitis
Epidemiology:
About one quarter of alliridocyclitiscases have a chronicclinical course.
Etiology:
See Table 8.1.
Symptoms:
See acute iridocyclitis. Chronic iridocyclitis
may exhibit minimalsymptoms.
Diagnostic considerations:
See acute iridocyclitis.
Differential diagnosis:
The disorder should be distinguished from
acuteglaucoma, conjunctivitis, and keratitis.
Complications:
Total obliteration of the pupil by posterior synechiae
isreferred to a pupillary block.
Because the aqueous humor can no longer circu-late, secondary angle closure glaucoma with iris bombé occurs. Occlusion ofthe pupil also results in
fibrous scarring in the pupil. This can lead to thedevelopment of posterior
subcapsular opacities in the lens (secondary
cata-ract). Recurrent iridocyclitis can also lead to calcific band
keratopathy.
Treatment:
In pupillary
block with a secondary angle closure glaucoma, aNd:YAG laser iridotomy may be performed to create a shunt to allow
theaqueous humor from the posterior chamber to circulate into the anterior
chamber. In the presence of a secondary
cataract, a cataract extraction
may be performed when the inflammation has abated.
Prognosis:
Because of the chronic recurrent course of the
disorder, itfrequently involves complications such as synechiae or cataract
that may progress to blindness from shrinkage of the eyeball.
Choroiditis
Epidemiology:
There are few epidemiologic studies of
choroiditis. Theannual incidence is assumed to be four cases per 100 000
people.
Etiology:
See Table 8.1.
Symptoms:
Patients are free of pain, although they
report blurred vision andfloaters.
Choroiditis is painless as the choroid is
devoid of sensory nerve fibers.
Diagnostic considerations:
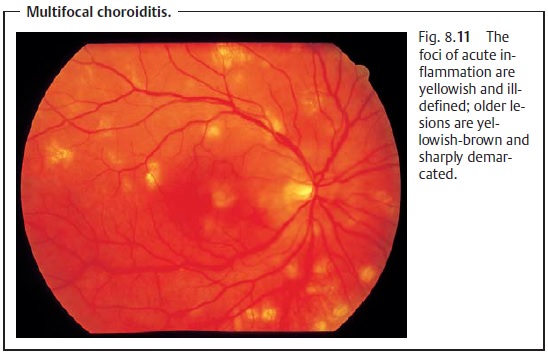
Ophthalmoscopy reveals isolated or multiplechoroiditis foci. In acute disease they appear as ill-defined white dots (Fig. 8.11). Once scarring has occurred the foci are sharply demarcated with a yellowish-brown color. Occasionally the major choroidal vessels will be vis-ible through the atrophic scars.
No cells will be found in the vitreous body in aprimary choroidal
process.However,
inflammation proceeding from the retina (retinochoroiditis) will exhibit cellular infiltration of the vitreous body.
Differential diagnosis:
This disorder should be distinguished from
retinalinflammations, which are accompanied by cellular infiltration of the
vitreous body and are most frequently caused by viruses or Toxoplasma gondii.
Treatment:
Choroiditis is treated either with antibiotics
or steroids, depend-ing on its etiology.
Prognosis:
The inflammatory foci will heal within two to
six weeks and formchorioretinal scars. The scars will result in localized
scotomas that will reduce visual acuity if the macula is affected.
Sympathetic Ophthalmia
Definition
Specific bilateral inflammation of the uveal
tract due to chronic irritation of one eye, caused by a perforating wound to
the eye or intraocular surgery, produces transferred uveitis in the fellow
eye.
Epidemiology:
Sympathetic ophthalmia is very rare.
Etiology:
Sympathetic uveitis can occur in anotherwise unaffected eyeevenyears after
penetrating injuries or intraocular surgery in the fellow eye, especially where
there was chronic irritation. Tissues in the injured eye (uveal tract, lens,
and retina) act as antigens and provoke an autoimmune dis-order in the
unaffected eye.
Symptoms:
The earliest symptoms include limited range of
accommodationand photophobia. Later there is diminished visual acuity and pain.
Diagnostic considerations:
Clinical symptoms include combined
injections,cells and protein in the anterior chamber and vitreous body,
papillary and ret-inal edema, and granulomatous inflammation of the choroid.
Differential diagnosis:
The disorder should be distinguished from
iridocycli-tis and choroiditis from other causes (see Table 8.1).
Treatment:
The injured eye, which is usually blind, must
be enucleated toeliminate the antigen. High-dose topical and systemic steroid
therapy is indi-cated. Concurrent treatment with immunosuppressives
(cyclophosphamide and azathioprine) may be necessary.
Clinical course and complications:
The disorder has a chronic clinical courseand may involve severe
complications of uveitis such as secondary glaucoma,
secondary cataract, retinal detachment, and
shrinkage of the eyeball. Sympa-thetic ophthalmia can lead to blindness in
particularly severe cases.
When the injured eye is blind, prophylactic
enucleation is indicated before the onset of sympathetic ophthalmia in the
fellow eye. An early sign of sympathetic ophthalmia is a limited range of
accommodation with photophobia.
Related Topics