Chapter: Essentials of Psychiatry: Social Psychology
Social Psychology: Interpersonal Processes: The Egoism-Altruism Debate
The Egoism–Altruism Debate
Historically, the Western perspective has been that
human be-ings tend to be motivated by self-interest (egoism). It is therefore
not surprising that investigators concerned with prosocial be-havior have
debated the veracity of the concept of altruistically motivated prosocial acts
in which others are benefited with no apparent short-term or long-term benefits
for the helper. A model proposed by Batson (1987, 1998) is intended to account
for altruism without invoking self-serving motives by establish-ing empathy as
a key factor that drives altruistic behavior. Ac-cording to this
empathy–altruism hypothesis, empathy provides a vehicle for adopting the
perspective of the other in need that then motivates the helper to act with the
goal of benefiting the other. Because empathic emotion is distinguished from
that of a distress response, it is argued that helpful acts resulting from
empathic determinants are carried out with the intention of enhancing the
welfare of the other rather than the self. Three types of self-serving motives
have been proposed to challenge the empathy–altruism hypothesis, including the
prospect of self and social rewards for providing help, avoidance of self or
social punishment for failing to help, and reduction of aversive arousal associated
with feelings of empathy. In reviewing existing re-search, Batson (1998)
concluded that none of these self-serving motives could adequately account for
the relationship between empathy and helping behavior, and that, on balance,
empirical findings generally support the empathy–altruism hypothesis that there
are instances of altruism that can be distinguished from helping behavior
involving self-serving motives. Batson (1998) further proposed a general model
involving four categories of prosocial motivation, each of which is linked to
specific val-ues. These include egoism (valuing self-enhancement), altruism
(valuing other-enhancement at the level of the individual), col-lectivism
(valuing other-enhancement at the level of the social group), and principlism
(valuing maintaining faithfulness to specific moral ideals). Although ideally
these four categories of prosocial motivation operate in cooperative and
complementary ways, they also may at times come into conflict. In
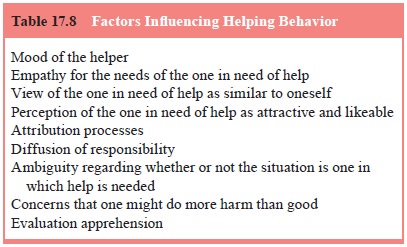
investigations of helping behavior, factors that influence whether or not an
in-dividual will engage in helping others, focus on characteristics of the
helper, the person who is in need of help, and the situation (Batson 1998)
(Table 17.8).
The high value placed on aiding those in ill-health
is ubiq-uitous in human life, exemplified at the cultural level by health care
professions and health care institutions entrusted to care for those in need of
medical intervention. Although multiple factors
contribute to the existence of health care
institutions and per-sonal decisions to work in health-related fields,
prosocial moti-vations are key among them. At the level of the individual, the
family and peer group, caring and empathy may propel the desire to help those
who are ill by providing emotional and instrumental support. As myriad
empirical investigations have shown, these prosocial acts of social support
provide beneficial health effects for individuals who receive them (Stroebe and
Stroebe, 1996).
Empathy engenders a sense of interest in and care
for oth-ers (Batson, 1998). The capacity for empathy is an important part of
healthy social relationships in that it enhances understanding of others and
thereby facilitates social connection and the sup-portive dimensions of
relationships. As such, clinical assessment should incorporate an evaluation of
empathy skills, especially in instances where clinical difficulties stem from
maladaptive rela-tional patterns. Consideration of the balance of empathic
versus self-serving interpersonal stances of the patient can be useful, not
only in individual psychotherapy but also in work with cou-ples seeking help in
resolving conflictual relationship patterns.
The clinical relevance of empathy extends to the
clinical practitioner. Therapist empathy is crucial to the understanding of the
patient and to the maintenance of the therapist’s concern for and desire to
enhance patient well-being. It is, therefore, hard to imagine the practice of
psychotherapy without empathic invest-ment of the therapist (Watson, 2002).
Although a powerful tool of therapeutic change, accurate empathy requires that
the thera-pist bear witness to considerable emotional pain in the process of
helping the patient. In some instances, the therapist may be overwhelmed by the
clinical issues of a given patient, and in re-sponse may retreat from an
empathic stance by distancing from, avoiding, or becoming numb to the
experience of the patient. It has been suggested that this empathic retreat is
a factor in the phenomenon of clinician burnout (Batson, 1998). As such,
em-pathic availability is an important variable for therapists to attend to in
their day-to-day work with patients.
Related Topics