Chapter: Essentials of Psychiatry: Social Psychology
Social Psychology: Interpersonal Processes: Attachment
Interpersonal Processes
Recent multidisciplinary trends in theory and research
on in-terpersonal phenomena have converged in scientific efforts to elucidate
relationship dynamics, including their antecedents and consequences (Reis et al., 2000). Underlying these efforts
is the assumption that, since human behavior takes place within a relational
context, a comprehensive scientific understanding of human behavior requires
careful study of interpersonal relation-ships (Reis et al., 2000). Although there have been differences of opinion
regarding how to define the term relationship, there is loose agreement that a
relationship involves an interaction be-tween relational partners that affects
the subsequent behavior of each partner in the interaction (Berscheid and Reis,
1998).
The study of interpersonal relationships spans a
multitude of behavioral domains relevant to social psychology. Although
recognition of the limits of the traditional individualistic focus of social
psychological theory and research recently has prompted calls for a more
systemic conceptual approach to research on in-terpersonal relationships, the
vast majority of work to date has examined relationships between individual
variables and rela-tionship experiences (Reis et al., 2000). It is important to empha-size that the nature and
qualities of human social interaction are not attributable solely to
evolutionary and biological influences and processes and are not directly
parallel to animal behavior (Hinde, 1987). Further, while an evolutionary
perspective can provide useful insights, adoption of such a viewpoint does not
imply strict genetic determinism or unmodifiability of evolved behavioral
patterns (Buss and Kenrick, 1998).
Attachment
Bowlby (1982) regarded attachment between infants
and caregiv-ers as an innate relational pattern that evolved in order to ensure
the survival of the infant. Attachment phenomena are common in birds and
mammals, with extended dependency periods in which offspring are fed, cleaned,
sheltered and protected by the parent. In many species, attachment is enhanced
by imprinting (Lorenz, 1970), a learned attachment that forms at the earliest
phases of development. Imprinting is most likely to occur dur-ing specific,
critical periods of development. If imprinting is not achieved during those
times, it is difficult to attain. Attachment facilitates survival of the
offspring, and investment in parental care for offspring is theorized to
involve a cost–benefit trade off; the increased likelihood that offspring will
survive is weighed against potential costs of parental care.
Attachment theory has as its cornerstone a system
of recip-rocal interactions that facilitate psychological safety and security
(i.e., attachment behavioral system) (Bowlby, 1973, 1980, 1982). According to
Bowlby’s theory of attachment, as a consequence of evolutionary processes,
children possess emotional and behavio-ral systems that organize and direct
them to seek proximity and to bond with their primary caretakers when they feel
distressed or threatened. The nature and quality of parental response in such
instances influences the child’s development. Children’s internal working
models of the attachment figure and the self in relation to this figure (i.e.,
self- and object-representations and schemas of interaction patterns between
self and attachment figures) influ-ence their attachment style and the quality
of their interpersonal relationships (Bretherton and Munholland, 1999).
The bulk of attachment research has been conducted
with young children and their primary caretakers. This research reveals four
attachment bonds types (i.e., secure, avoidant, anxious/ambivalent,
disorganized/disoriented) most noted when
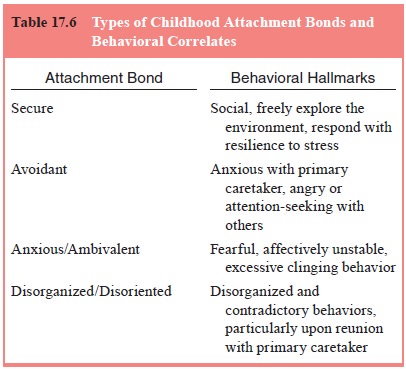
infants and their primary caretaker are reunited
following a brief, experimentally controlled separation (Ainsworth et al., 1978; Hesse and Main, 2000;
Main, 2000) (Table 17.6).
Securely attached children are social, able to
explore their environment freely, and resilient when faced with stressful
situa-tions. In contrast, avoidant children tend to be anxious with their
primary caretaker(s) and angry or attention-seeking with others.
Anxious/ambivalent children typically are fearful of the envi-ronment,
affectively unstable, and cling inordinately to others. Finally, disorganized/disoriented
children often exhibit signs of disorganization and contradictory behaviors,
particularly upon reunion with their primary caretaker. Longitudinal research
shows that attachment behavior patterns are stable over time, predictive of
school behavior and peer interactions, and consist-ent with the quality of
parenting received and parental attach-ment style (Bowlby, 1988; Sroufe, 2002;
Sroufe et al., 1990).
Adult Attachment
Recently, clinicians and researchers have begun to
turn their attention to attachment patterns in adults (Sperling and Berman,
1994; West and Sheldon-Keller, 1994). Similar to infant attachment patterns,
adult attachment is presumed to be rooted in evolutionarily significant
biological adaptation processes (Hazan and Diamond, 2000) and is characterized
by a strong interest in the other, a desire to remain physically close to and
spend time with the other, reliance on ongoing access to the other, dependence upon
the other for support in the face of physical or emotional threats, and
feelings of discomfort and distress upon separation (Feeney, 1999; Shaver and
Hazan, 1993; West and Sheldon-Keller, 1994). However, unlike attachment
patterns in children, the primary adult attachment objects typically are peers,
adult patterns of relating are more reciprocal, and attachment figures often
also are sexual partners (Feeney et al.,
2000). Adult attachment is influenced significantly by working models of the
attachment object and self that have their origins in childhood attachment
experiences with primary caretakers (Bartholomew and Horowitz, 1991). Work in
adult attachment theory addresses the establishment and maintenance of primary
emotional partnerships in adult life, the effects of early and current
attachment experiences on the development of psychopathology, and the use of
attachment theory to guide therapeutic interventions.
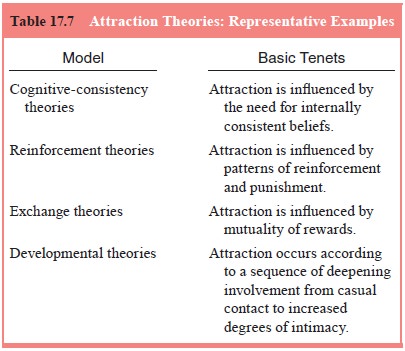
Among the most compelling questions in research on
close relationships are those that pertain to relationship sat-isfaction and
stability. Work in this area has been influenced (see Table 17.7) heavily by
the social exchange tradition, which assumes that the exchange of rewards and
costs is a key influ-ence on relationships (Berscheid and Reis, 1998).
Specifically, social exchange theory suggests that people are motivated to
maximize rewards and minimize costs, with the favorability of relational
outcomes being defined by the relative balance of rewards and costs for each
relationship participant. Within the social exchange framework, interdependence
theory (Thibaut and Kelley, 1959; Rusbult and Van Lange, 1996) has been
especially useful in making predictions about relationship satisfaction and
stability. This model posits that people evalu-ate relationship satisfaction
according to expectancy standards for relationship outcomes (comparison level),
and that relation-ship satisfaction is a function of the extent to which
outcomes meet or exceed these expectancy standards. The model also posits an
additional evaluative standard employed by individu-als to determine whether or
not to stay in a given relationship (comparison level for alternatives). This
standard is relevant to predicting relationship stability, as it represents the
mini-mal acceptable relationship outcome level for remaining in a given
relationship when outcomes associated with available alternative relationships
are taken into consideration. Accord-ing to the model, therefore, relationship
stability is related to the combined influence of relationship attractiveness
and the availability of desirable alternatives external to the relation-ship.
Relationship stability is likely to be compromised to the extent that
relationship attractiveness is lower than the appeal of available relationship
alternatives. In general, relation-ship stability is influenced by degree of
commitment to the relationship, availability in the social environment of
viable re-lationship alternatives, perceived approval for the relationship by
the social networks of the respective partners, and partner perceptions of the
relative equity/inequity in gains as a result of being in the relationship
(Berscheid and Reis, 1998).
Sexual behavior is an important channel of
expression in certain types of interpersonal relationships (e.g., romantic
relationships) and its patterns of expression may symbolize underlying
relational dynamics (Mason, 1991). While some social psychological perspectives
have explored sexuality as it relates to romantic love, much of the extant theory
and research related to sexuality has focused on mate selection (Berscheid and
Reis, 1998). Evolutionary psychology, in particular, has exam-ined mate
selection in detail (Buss and Kenrick, 1998).
In humans, sexual behavior serves more than the
purely biological functions of procreation and physiological release, as it is
also an important means of expressing love, closeness and the need for human
contact. Sexual behavior is manifested in diverse ways determined by a complex
interplay among one’s relationships, life situations and the broad
sociocultural context. Although normative sexual behavior has received
systematic em-pirical study, beginning with the survey research of Kinsey and
colleagues (1948, 1953) and continuing to the present day (Janus and Janus,
1994), much of the emphasis of psychological research has been on sexual
dysfunction and its treatment (Kaplan, 1974; Masters and Johnson, 1970).
Considerable evidence has accrued that social integration in general, and social support in particular, are related both to en-hanced health and lowered risk of mortality (Berscheid and Reis, 1998; Stroebe and Stroebe, 1996). Both main effect models and stress-buffering models have been employed to explain observed relationships between social support and health factors (Stroebe and Stroebe, 1996). Main effect models assume that a specific factor, such as social influence, may directly affect health and well-being via its impact on health beliefs, attitudes and behav-ior. By contrast, stress-buffering models presume that social sup-port confers health benefits only to the extent that an individual is experiencing stress. According to this perspective, social support may provide health benefits indirectly by serving as a resource to help the individual cope with health-related stress.
Several factors influence the likelihood of
social-support provision. Among these are social-exchange processes and so-cial
norms surrounding provision of help for individuals in ill-health, as well as
causal attributions made about the recipient of social support (Stroebe and
Stroebe, 1996). For example, social psychological research suggests that a
curvilinear relationship exists between degree of distress and likelihood of an
individual receiving social support, with moderate distress eliciting the
greatest degree of supportive actions by others. Further, indi-viduals
perceived by others as responsible for their plight may be less likely to
receive social support than those whose ill-health is perceived by others as
caused by uncontrollable circumstances. Additionally, social support may be
withheld if individuals are perceived as not trying hard enough to manage their
illness or are not showing sufficient improvement in response to social support
provision. These patterns may have unfortunate implications for individuals
with disease syndromes that cause high stress levels, are highly stigmatized,
and/or are chronic or progressive, as they may find themselves socially
isolated at times of high need for social contact.
As has already been mentioned, there is a vast
scientific literature in support of the idea that relationships contribute both
to physical and mental well-being (Berscheid and Reis, 1998; Reis et al., 2000; Stroebe and Stroebe,
1996). This em-pirical base complements the widespread clinical regard for the
treatment relationship as a primary tool of influence and thera-peutic change
(Mitchell, 2000). As such, social psychological theory and research on
relationships can contribute substan-tively to current thinking about how to
structure the clini-cian–patient relationship to maximize mental health
treatment benefit (Derlega et al.,
1991).
Related Topics