Chapter: Essentials of Psychiatry: Sexual Disorders
Sexual Disorders
Sexual Disorders
A wide array of sexuality topics impact psychiatry. These top-ics range
from those constituting a major social burden, such as teenage pregnancy, sex
crimes and sexually transmitted diseases, to those involving ethical and moral
values, such as abortion, extramarital affairs, commercial sex industries and
crossing sexual boundaries with patients. They include those with a
developmental or medical focus, such as sexual dysfunc-tion or sexual
dysfunction due to substance abuse or medical conditions, and those involving
lifestyles, such as sexual mi-nority status and drugs for sexual enhancement.
There are also those that center on psychiatry’s undisputed responsibility,
such as psychotropic medication-induced sexual dysfunction and the sexual
consequences of psychiatric illness. No discipline, no ideology, no religion
and certainly no textbook is suffi-cient fully to understand and encompass the
myriad expressions of human sexuality.
Psychiatry has known for almost a century that child de-velopment lays
the foundation for a wide variety of adult sexual outcomes (Freud, 1905). These
are reflected in the variations of gender, orientation, intention and ease of
sexual expression with chosen partners. Psychiatry has also been long aware
that the conduct of adolescent and adult sexual life is laden with concern, and
sometimes anguish, in every person. In the last generation, we have acquired
greater convictions about the profound public health implications of several
sexual patterns. First came aware-ness of the high incidence of childhood
sexual abuse and its long-term consequences. Then came the data showing that
some psychiatrists and other trusted professionals engaged in genital
intimacies with patients. Psychiatry responded by unambigu-ously clarifying our
ethical standards. At about the same time the AIDS epidemic led to a greater
awareness of the lives of ho-mosexual and bisexual men. In the 1990s when the
Internet us-age grew without regulation, addictions to at-home pornography
appeared. As the use of SSRIs became widespread, psychiatrists learned about
their negative sexual impact. In 1998 an effective pill for erectile
dysfunction created an explosion of media inter-est across the world. The
Viagra story reminded us that sexual function is really important to people.
Psychiatry prides itself about being the only field that can comprehend
the biopsychosocial aspects of illness. We under-stand that all sexual
expression is simultaneously constituted by biological, psychological and
social forces. We also know that sexual disorders are a high prevalence, high
incidence source of personal suffering, affecting almost every person at some
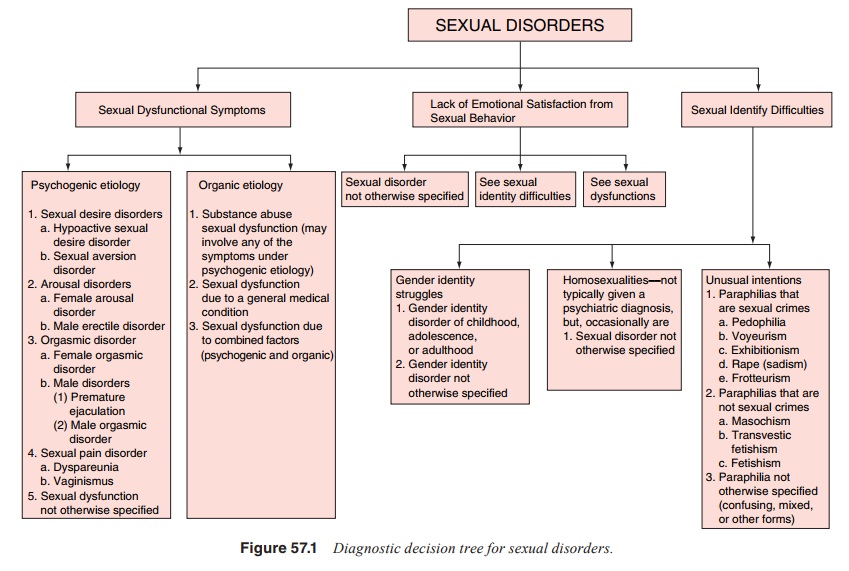
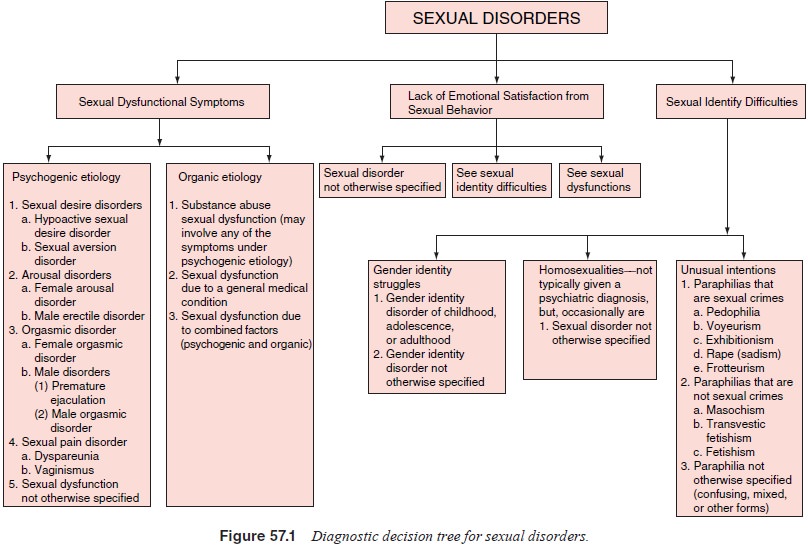
time in the life-cycle. Sexual disorders often play a subtle role in the
genesis of other psychiatric disorders as presented in Figure 57.1
Patients assume their psychiatrists know about sexuality. Therapists can
be helpful to many individuals and couples with these problems if they have an
interest in the area, a comfort with the subject and a modest fund of
knowledge. Sometimes the help can be given quite efficiently. The assistance is
often based on knowledge of the diverse origins of these problems. To be able
to treat a broad range of sexual disorders the psychiatrist needs to be
diagnostically competent, skillful with medications and will-ing to engage in
psychotherapeutic processes.
The Components of Sexuality
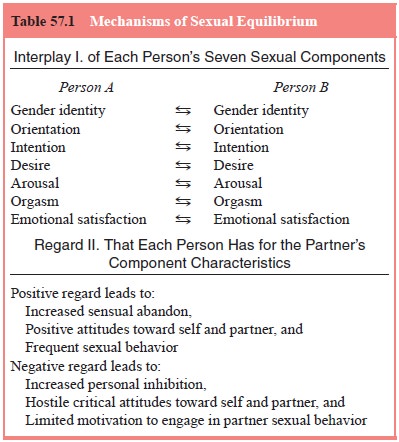
An adult’s sexuality has seven components – gender identity,
ori-entation, intention (what one wants to do with a partner’s body and have
done with one’s body during sexual behavior), desire, arousal, orgasm and
emotional satisfaction. The first three com-ponents constitute our sexual
identity. The second three com-prise our sexual function. The seventh,
emotional satisfaction, is based on our personal reflections on the first six
(Table 57.1). The DSM-IV-TR designates impairments of five of these compo-nents
as pathologies. Variations in orientation and the failure to find ordinary
sexual experience emotionally satisfying, although problems for some, are not
designated as “disorders”.
Sexual Development Through the Life-cycle
While the psychological foundations for a healthy sexual life are laid down during childhood through parent–child relationships, each subsequent phase of life – adolescence, young adulthood, middle-life, and older age – has inherent developmental chal-lenges and potentials. The normal tasks of sexual development at each phase provide the clinician with an understanding of age-related etiologies of sexual disorders. Adolescent sexual trou-bles often reflect difficulties consolidating a personally accept-able sexual identity. Young adult dysfunctions often indicate the presence of psychological obstacles to growing comfortable as a sexual pleasure-seeking, pleasure-giving person while integrat-ing sex into the larger context of human attachment. Middle-life disorders often represent failures to maintain psychologi-cal intimacy and diplomatically to negotiate tensions within an increasingly complex interpersonal relationship. The dysfunc-tions of older persons often represent failures to preserve sexual function in the face of biological assaults of menopause, aging, illness, medications, radiation and surgery. Most etiologic fac-tors can operate in another epoch as well. For instance, a young person’s new indifference to sexual behavior may be due to an SSRI or an older person’s new marriage may expose previously avoided personal discomfort with receiving and giving sexual pleasure
Related Topics