Chapter: Essentials of Psychiatry: Sleep and Sleep-Wake Disorders
Role of the Sleep Laboratory in Clinical Sleep Disorders
Role
of the Sleep Laboratory in Clinical Sleep Disorders
Psychiatrists
can usually diagnose most sleep disorders by tra-ditional, simple but
systematic clinical methods. Referral to a specialized sleep disorders center,
however, should be consid-ered in patients suspected of having severe
intractable insomnia, persistent excessive daytime sleepiness and sleep
disorders due to a general medical condition (such as narcolepsy, REM sleep
behavior disorder, sleep apnea, periodic limb movements in sleep [PLMS], or sleep-related
epilepsy). Specialists in sleep disorders medicine will evaluate the patient
and, if necessary, arrange for sleep laboratory or ambulatory diagnostic
procedures.
One of
the most important and common laboratory exami-nations is all-night
polysomnography, which typically records the EEG activity’s eye movements with
the electrooculogram, and muscle tone with the electromyogram from the chin
(submental) muscles. These measures are used to determine sleep stages
visu-ally scored as 20- or 30-second epochs by a sleep technician. To evaluate
sleep-related respiration and cardiovascular function, measures are made of
nasal and oral air flow with a thermistor; of sounds of breathing and snoring
with a small microphone near the mouth; of respiratory movements of the chest
and abdominal walls; of heart rate with the electrocardiogram; and of
blood-oxy-gen saturation with finger oximetry. To evaluate PLMS, an
elec-tromyogram from the shin (anterior tibial) muscles is obtained. Other more
specialized tests include intraesophageal pressures, which increase during the
upper airway resistance syndrome if respiration is impeded, nocturnal penile
tumescence in the evalu-ation of impotence and core body temperature (usually
rectal or tympanic membrane).
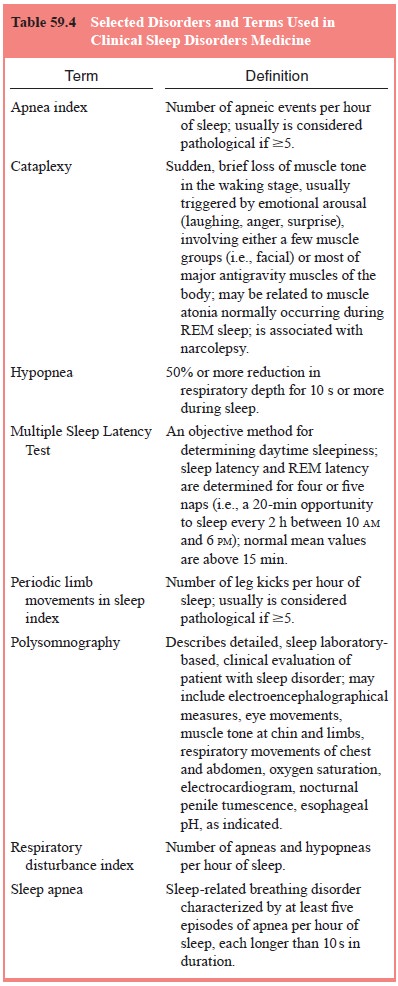
Daytime
sleepiness can be evaluated in the sleep labora-tory with the Multiple Sleep
Latency Test, which measures sleep latency during opportunities for napping
during the day (see Table 59.4). In addition, subjective sleepiness can be
assessed by
a
questionnaire, the Stanford Sleepiness Scale, in which the sub-ject rates
sleepiness on a 7-point scale at set intervals throughout the day
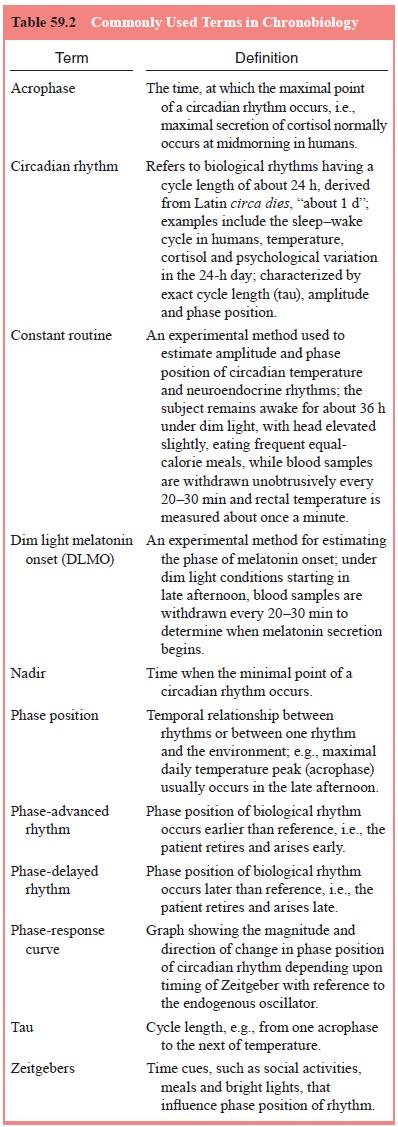
.Two
research laboratory procedures have been developed for experimental measurement
of circadian phase in humans: the constant routine method for temperature and
neuroendocrine secretions, and the dim light melatonin onset method for
mela-tonin (see Table 59.2).
According
to DSM-IV-TR definitions (American Psychiat-ric Association, 1994), primary
sleep disorders are presumed to arise from endogenous abnormalities in
sleep–wake-generating mechanisms, timing mechanisms, sleep hygiene, or
conditioning, rather than occurring secondary to medical or psychiatric
disor-ders. Two types of primary sleep disorders are defined: dyssom-nias (abnormalities in the
amount, quality, or timing of sleep) and
parasomnias (abnormal behaviors associated with sleep, such as nightmares
or sleepwalking). In addition, sleep disorders may be related to other mental
disorders, general medical conditions, and substance abuse.
Related Topics