Chapter: Essentials of Psychiatry: Sleep and Sleep-Wake Disorders
General Approach to the Patient with a Sleep Disorder
General
Approach to the Patient with a Sleep Disorder
Disorders
of sleep and wakefulness are common. Insomnia com-plaints are reported by about
one-third of adult Americans during a 1-year period; clinically significant
obstructive sleep apnea may be seen in as many as 10% of working, middle-aged
men; and sleepiness is an underrecognized cause of dysphoria, automobile
accidents and mismanagement of patients by sleep-deprived physicians. Nearly
all physicians will hear complaints of sleep problems. Psychiatrists may be
even more likely than other medical specialists to receive these complaints. Of
particular importance for mental disorders, prospec-tive epidemiological
studies suggest that persistent complaints of either insomnia or hypersomnia
are risk factors for the later onset of depression, anxiety disorders and
substance abuse.
This
attempts to provide a framework for psychia-trists and other mental health
specialists to use in understand-ing the multiple causes of the sleep
disorders, their diagnostic evaluation and their treatment. To assist the
patient with a sleepcomplaint, the psychiatrist needs to have a diagnostic
frame-work with which to obtain the information needed about both the patient
as a person and his or her disorder. Two issues are particularly important: 1)
How long has the patient had the sleep complaint? Transient insomnia and
short-term insomnia, for example, usually occur in persons undergoing acute
stress or other disruptions, such as admission to a hospital, jet lag,
be-reavement, or change in medications. Chronic sleep disorders, on the other
hand, are often multidetermined and multifaceted: 2) Does the patient suffer
from any preexisting or comorbid disorders? Does another condition cause the
sleep complaint, modify a sleep complaint, or affect possible treatments? In
gen-eral, because common sleep disorders are frequently secondary to underlying
causes, treatment should be directed at underlying medical, psychiatric,
pharmacological, psychosocial, or other disorders.
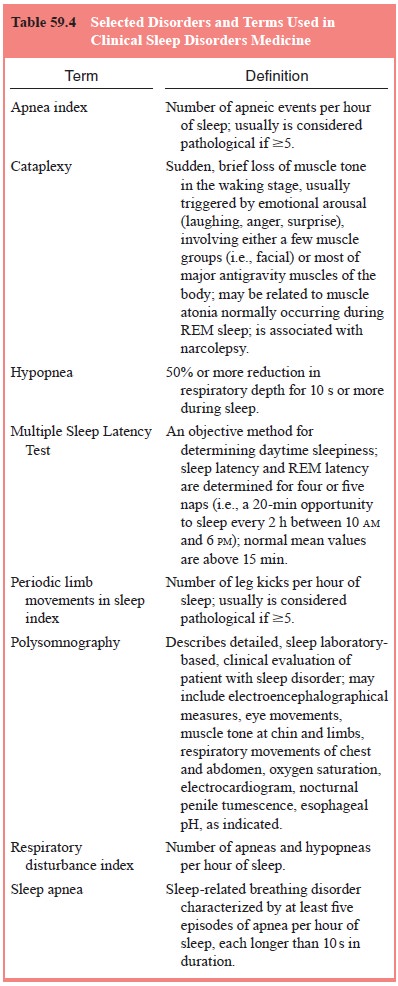
A
detailed history of the complaint and attendant symp-toms must be obtained
(Tables 59.3 and 59.4). Special atten-tion should be given to the timing of
sleep and wakefulness; qualitative and quantitative subjective measures of
sleep and wakefulness; abnormal sleep-related behaviors; respiratory
difficulties; medications or other substances affecting sleep, wakefulness, or
arousal; expectations, concerns, attitudes about sleep, and efforts used by the
patient to control symp
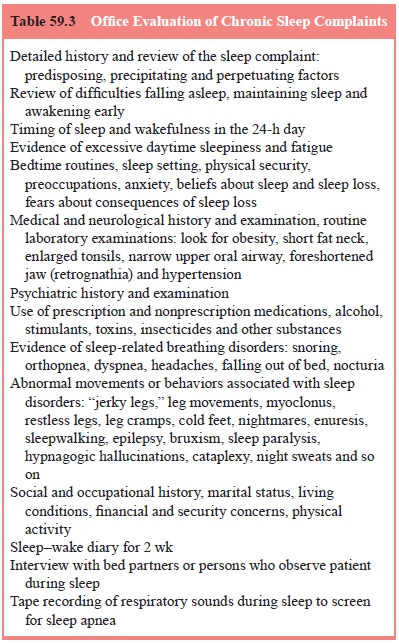
toms; and
the sleep–wake environment. The psychiatrist must be alert to the possibility
that sleep complaints are somatic symptoms, which reflect individual ways of
experiencing, expressing and coping with psychosocial distress, stress, or
psychiatric disorders
Sleep
disorders vary with age and gender and, possibly, with culture and social
class. As mentioned previously, the circa-dian timing of rest–activity, sleep
duration at night, and daytime napping and sleepiness vary with age and gender.
In addition, parasomnias are most common in boys, Kleine–Levin syndrome in
adolescent boys, delayed sleep phase syndrome in adolescents and young adults,
insomnia in middle-aged and elderly women, REM sleep behavior disorder and
sleep-related breathing disor-ders in middle-aged men, and advanced sleep phase
syndrome in the elderly. Sleep–wake patterns are also influenced by cultural or
geographical factors, such as the siesta and late bedtime com-monly associated
with tropical climates, or the winter hypersom-nia and summer hyposomnia said
to occur near the Arctic circle. Insomnia is more common in lower than in
middle and upper socioeconomic classes, perhaps reflecting the stress of
poverty, crowding and lack of privacy, poor medical care, drugs and alco-hol,
lack of physical security and so forth.
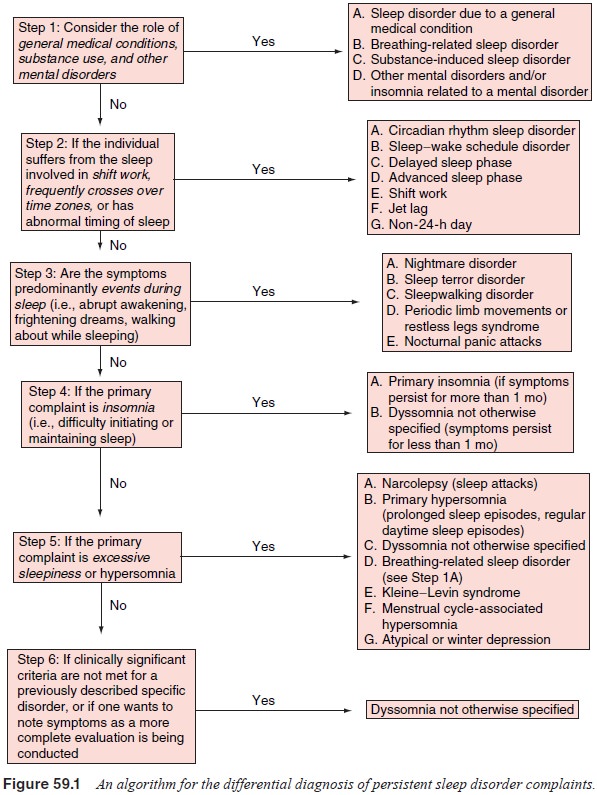
One
approach to the differential diagnosis of persistent sleep disorders is
suggested in the algorithm in Figure 59.1. First, determine whether the sleep
complaint is due to another medical, psychiatric, or substance abuse disorder.
Secondly, consider the role of circadian rhythm disturbances and sleep
disorders associ-ated with abnormal events predominantly during sleep. Finally,
evaluate in greater detail complaints of insomnia (difficulty initi-ating or
maintaining sleep) and excessive sleepiness.
Related Topics