Chapter: Clinical Anesthesiology: Anesthetic Equipment & Monitors : Breathing Systems
Resuscitation Breathing Systems
RESUSCITATION BREATHING SYSTEMS
Resuscitation bags (AMBU bags or
bag-mask units) are commonly used for emergency ventilation because of their
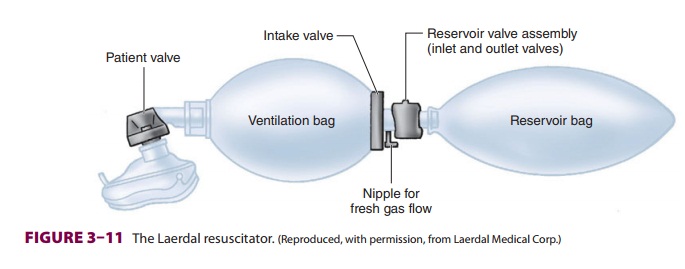
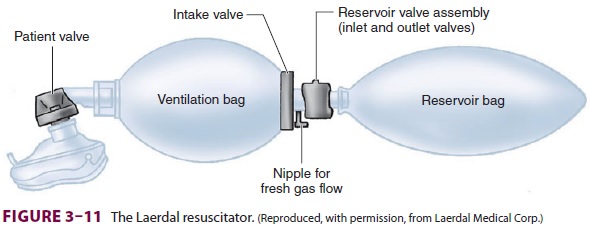
simplicity, portability, and ability to deliver almost 100% oxygen (Figure 3–11).
A resuscitator is unlike a Mapleson
circuit or a circle system because it contains a nonrebreathing valve. (Remember that a Mapleson system is
considered valveless even though it contains an APL valve, whereas a circle
system contains unidirectional valves that direct flow through an absorber but
allow rebreathing of exhaled gases.)
High concentrations of oxygen can be
delivered to a mask or tracheal tube during spontaneous or controlled
ventilation if a source of high fresh gas flow is connected to the inlet
nipple. The patient valve opens during controlled or spontaneous inspi-ration to
allow gas flow from the ventilation bag to the patient. Rebreathing is
prevented by venting exhaled gas to the atmosphere through exhalation ports in
this valve. The compressible, self-refilling ventilation bag also contains an
intake valve. This valve closes during bag compression, permitting
positive-pressure ventilation. The bag is refilled by flow through the fresh
gas inlet and across the intake valve. Connecting a reservoir to the intake
valve helps prevent the entrainment of room air. The reservoir valve assembly
is really two unidirectional valves: the inlet valve and the outlet valve. The
inlet valve allows ambient air to enter the ventilation bag if fresh gas flow
is inadequate to maintain reservoir filling. Positive pressure in the reservoir
bag opens the outlet valve, which vents oxygen if fresh gas flow is excessive.
There are several disadvantages to
resuscitator breathing systems. First, they require high fresh gas flows to
achieve a high Fio2. Fio2 is directly pro-portional to
the oxygen concentration and flow rate of the gas mixture supplied to the
resuscitator (usually 100% oxygen) and inversely proportional to the minute
ventilation delivered to the patient. For example, a Laerdal resuscitator
equipped with a res-ervoir requires a flow of 10 L/min to achieve an inspired
oxygen concentration approaching 100% if a patient with a tidal volume of 750
mL is ventilated at a rate of 12 breaths/min. The maximum achievable tidal
volumes are less than those that can be achieved with a system that uses a 3-L
breathing bag. In fact, most adult resuscitators have a maximum tidal vol-ume
of 1000 mL, which is sufficient for the lower tidal volumes generally employed
in patient management. Finally, although a normally functioning patient valve
has low resistance to inspiration and expiration, exhaled moisture can cause
valve sticking.
Related Topics