Chapter: Medical Physiology: Pituitary Hormones and Their Control by the Hypothalamus
Regulation of Growth Hormone Secretion
Regulation of Growth Hormone Secretion
For many years it was believed that growth hormone was secreted primarily during the period of growth but then disappeared from the blood at adolescence. This has proved to be untrue. After adolescence, secretion decreases slowly with aging, finally falling to about 25 per cent of the adolescent level in very old age.
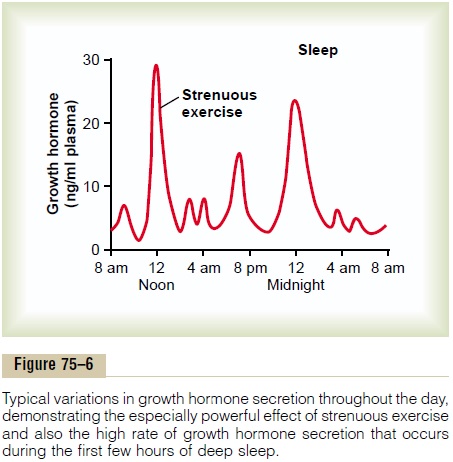
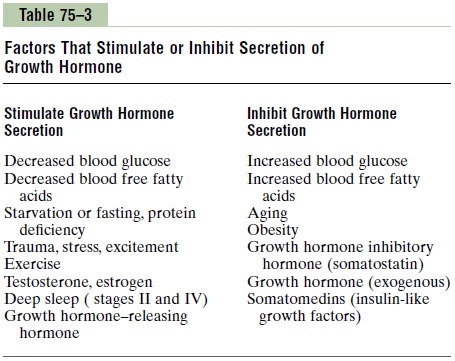
Growth hormone is secreted in a pulsatile pattern, increasing and decreasing. The precise mechanisms that control secretion of growth hormone are not fully understood, but several factors related to a person’s state of nutrition or stress are known to stimulate secretion: (1) starvation, especially with severe proteindeficiency; (2) hypoglycemia or low concentration of fatty acids in the blood; (3)exercise; (4) excitement; and (5) trauma. Growth hormone also characteristically increases during the first 2 hours of deep sleep, as shown in Figure 75–6. Table 75–3 summarizes some of the factors that are known to influence growth hormone secretion.
The normal concentration of growth hormone in the plasma of an adult is between 1.6 and 3 ng/ml; in a child or adolescent, it is about 6 ng/ml. These values often increase to as high as 50 ng/ml after depletion of the body stores of proteins or carbohydrates during prolonged starvation.
Under acute conditions, hypoglycemia is a far more potent stimulator of growth hormone secretion than is an acute decrease in protein intake. Conversely, in chronic conditions, growth hormone secretion seems to correlate more with the degree of cellular protein depletion than with the degree of glucose insufficiency. For instance, the extremely high levels of growth hormone that occur during starvation are closely related to the amount of protein depletion.
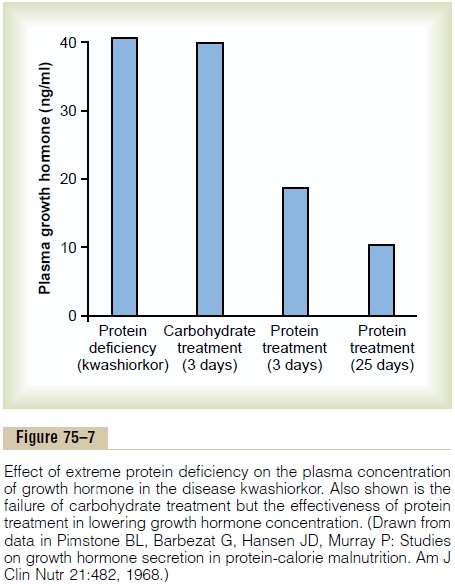
Figure 75–7 demonstrates the effect of protein defi-ciency on plasma growth hormone and then the effect of adding protein to the diet. The first column shows very high levels of growth hormone in children with extreme protein deficiency during the protein malnu-trition condition called kwashiorkor; the second column shows the levels in the same children after 3 days of treatment with more than adequate quantities of carbohydrates in their diets, demonstrating that the carbohydrates did not lower the plasma growth hormone concentration. The third and fourth columns show the levels after treatment with protein supple-ments for 3 and 25 days, respectively, with a concomi-tant decrease in the hormone.
These results demonstrate that under severe condi-tions of protein malnutrition, adequate calories alone are not sufficient to correct the excess production of growth hormone. The protein deficiency must also be corrected before the growth hormone concentration will return to normal.
Role of the Hypothalamus, Growth Hormone–Releasing Hormone, and Somatostatin in the Control of Growth Hormone Secretion
From the preceding description of the many factors that can affect growth hormone secretion, one can readily understand the perplexity of physiologists as they attempt to unravel the mysteries of regulation of growth hormone secretion. It is known that growth hormone secretion is controlled by two factors secreted in the hypothalamus and then transported to the anterior pituitary gland through the hypothalamic-hypophysial portal vessels. They are growthhormone–releasing hormone and growth hormone inhibitory hormone (also called somatostatin). Both ofthese are polypeptides; GHRH is composed of 44 amino acids, and somatostatin is composed of 14 amino acids.
The part of the hypothalamus that causes secretion of GHRH is the ventromedial nucleus; this is the same area of the hypothalamus that is sensitive to blood glucose concentration, causing satiety in hyper-glycemic states and hunger in hypoglycemic states. The secretion of somatostatin is controlled by other nearby areas of the hypothalamus. Therefore, it is reasonable to believe that some of the same signals that modify a person’s behavioral feeding instincts also alter the rate of growth hormone secretion.
In a similar manner, hypothalamic signals depicting emotions, stress, and trauma can all affect hypothala-mic control of growth hormone secretion. In fact, experiments have shown that catecholamines, dopamine, and serotonin, each of which is released by a different neuronal system in the hypothalamus, all increase the rate of growth hormone secretion.
Most of the control of growth hormone secretion is probably mediated through GHRH rather than through the inhibitory hormone somatostatin. GHRH stimulates growth hormone secretion by attaching to specific cell membrane receptors on the outer surfaces of the growth hormone cells in the pituitary gland. The receptors activate the adenylyl cyclase system inside the cell membrane, increasing the intracellular level of cyclic adenosine monophosphate (cAMP). This has both a short-term and a long-term effect. The short-term effect is to increase calcium ion transport into the cell; within minutes, this causes fusion of the growth hormone secretory vesicles with the cell membrane and release of the hormone into the blood. The long-term effect is to increase transcription in the nucleus by the genes to stimulate the synthesis of new growth hormone.
When growth hormone is administered directly into the blood of an animal over a period of hours, the rate of endogenous growth hormone secretion decreases. This demonstrates that growth hormone secretion is subject to typical negative feedback control, as is true for essentially all hormones. The nature of this feed-back mechanism and whether it is mediated mainly through inhibition of GHRH or enhancement of somatostatin, which inhibits growth hormone secre-tion, are uncertain.
In summary, our knowledge of the regulation of growth hormone secretion is not sufficient to describe a composite picture. Yet, because of the extreme secre-tion of growth hormone during starvation and its important long-term effect to promote protein syn-thesis and tissue growth, we can propose the follow-ing: the major long-term controller of growth hormone secretion is the long-term state of nutrition of the tissues themselves, especially their level of protein nutrition. That is, nutritional deficiency or excess tissue need for cellular proteins—for instance, after a severe bout of exercise when the muscles’ nutritional status has been taxed—in some way increases the rate of growth hormone secretion. Growth hormone, in turn, promotes synthesis of new proteins while at the same time conserving the proteins already present in the cells.
Related Topics