Chapter: Modern Medical Toxicology: Hydrocarbons and Pesticides: Pesticides
Pyrethrins and Pyrethroids - Insecticide
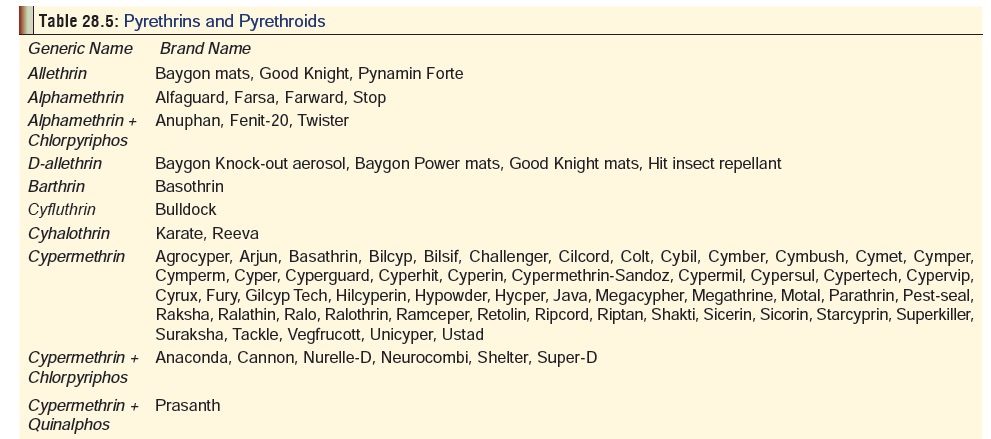
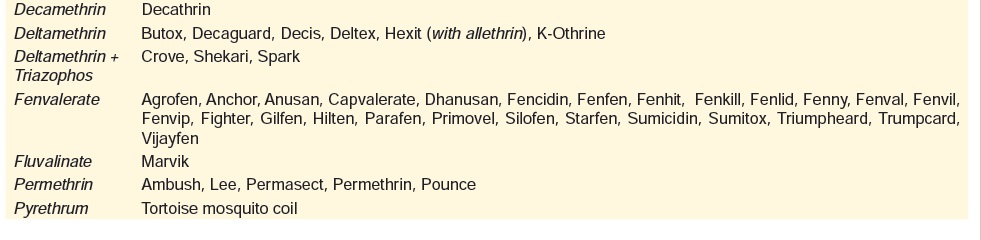
Pyrethrins and Pyrethroids
Pyrethrins
are active extracts of the chrysanthemum plant (Chrysanthemum cinerariaefolium), and include pyrethrum and
piperonyl butoxide. They are esters of pyrethric and chry-santhemic acids
formed by the keto alcohols pyrethrolone, cinerolone, and jasmololone.
Pyrethrin I and pyrethrin II are two of the most insecticidally potent
pyrethric and chrysan-themic esters. Pyrethroids are synthetic analogues and
number over 1000 varieties which are used as insecticides to incapaci-tate or
“knock out” insects. Most mammals are resistant since they can rapidly
metabolise and detoxify these agents. Common pyrethrins and pyrethroids
available commercially in India are mentioned in Table 28.5.
Uses
■■ These compounds are
used as household insect repellants and insecticides. They are sold as liquids,
sprays, dusts, powders, mats, and coils.
■■ They are also used
to prevent pest infestation in granaries, and in agriculture as pesticides.
■■ Pyrethrum extract is
effective for treating pediculosis of the head, body and pubic area.
Usual Fatal Dose
·
Pyrethrum has an LD50 of over 1
gm/kg. However, the minimal lethal dose of pyrethrum is not clearly
established, though it is probably in the range of 10 to 100 grams. Most cases
of toxicity are actually the result of allergic reactions.
Mode of Action
Structurally, pyrethroids are of 2
types—
Type I pyrethroids do not contain a cyano group, e.g. permethrin.
Type II pyrethroids contain a cyano group, e.g. deltame-thrin,
cypermethrin, fenpropathrin, fenvalerate, etc.
Like DDT, pyrethroids prolong the
inactivation of the sodium channel by binding to it in the open state. Type II
agents are more potent in this regard, and also act by inhibiting GABA-mediated
inhibitory chloride channels. Low toxicity in mammals is probably due to rapid
metabolic breakdown in the liver: pyrethrum is broken down mainly by oxidation
of the isobutenyl side chain of the acid moiety and of the unsaturated side
chain of the alcohol moiety with ester hydrolysis playing a role. Some
organophosphates may enhance pyrethrin toxicity due to competition for
carboxyesterases responsible for rapid detoxification of pyrethrins via ester
hydrolysis. Very young children are perhaps more susceptible to poisoning by
pyre-throids because they may not hydrolyse the pyrethrum esters efficiently.
Two types of allergens present in crude pyrethrum oleoresin have been identified: glycoproteins or glycopeptides ranging in molecular weight from 60,000 to 200,000 (most important) and the sesquiterpene lactones, principally pyrethrosin (minor importance). Refined pyrethrins and synthetic pyrethroids are said to have little or no allergenic effect.
Clinical Features
·
Skin
contact: dermatitis, blistering. The usual lesion is amild
erythematous dermatitis with vesicles, papules in moist areas, and intense
pruritus; a bulbous dermatitis may also occur. Skin contamination with
pyrethrins can cause localised paraesthesia.
·
Eye
contact: Eye exposures may result in mild to severecorneal damage
that generally resolves with conservative care. Corneal denudation and
decreased visual acuity have been reported following ocular contact exposure
during normal use of pediculicide shampoos containing pyrethrin. Chemical
conjunctivitis was diagnosed in a patient after a pyrethrin-containing mist was
inadvertently sprayed into the eyes.
·
Inhalation:
rhinorrhoea, sore throat, wheezing, dyspnoea.Asthma or reactive airways disease
syndrome can occur following inhalation exposures, as also hypersensitivity
pneumonitis with chest pain, cough, dyspnoea and bron-chospasm. Eosinophilia
may accompany an acute allergic reaction. Dizziness and headache have been
reported following exposure to pesticide mists.
·
Ingestion
(large doses): paraesthesias, nausea, vomiting,vertigo,
fasciculations, hyperthermia, altered mental status, seizures, pulmonary
oedema, coma. Nausea,vomiting and abdominal pain commonly occur and develop
within 10 to 60 minutes following ingestion. Hypotension and tachycardia,
associated with anaphy-laxis, may occur. Severe poisoning may result in marked
adrenal activation, with increases in adrenaline and noradrenaline accompanying
motor signs.
Diagnosis
·
Serum cholinesterase levels are
normal.
·
ECG may demonstrate ST-T changes,
sinus tachycardia, and ventricular premature beats.
·
A colour test with 2-2
(2-aminoethylamine) ethanol produces red to violet colour in the presence of
pyre-throidal substances. It is however not suitable for analysis of pyrethrins
in body fluids, except, possibly at very high concentrations.
Treatment
Skin contact—decontaminate with soap and water.
Eye contact—irrigate with normal saline or water for 10 to15 minutes.
Systemic poisoning—
·
Mild to moderate allergic reactions may be treated with
antihistamines (e.g. diphenhydramine 50 mg orally, intravenously, or
intramuscularly initially, then 25 to 50 mg orally every 4 to 6 hours for 24 to
72 hours) with or without inhaled beta agonists, corticosteroids (e.g methyl
prednisolone 1 to 2 mg/kg intravenously every 6 to 8 hours) or adrenaline
(1:10,000 solution, 3 to 5 ml diluted in 10 ml 0.9% saline slow intravenous
push over 5 to 10 minutes). Treatment of severe anaphylaxis also includes
oxygen supplementation, aggressive airway management, adrenaline, ECG
monitoring and IV fluids.
·
In massive ingestions, stomach wash can be done after making
sure that there are no petroleum distillate addi-tives.
·
Activated charcoal is beneficial. However, if the pyre-thrin
is formulated in an organic solvent, activated charcoal is unlikely to be of
benefit. If the pyrethrin is formulated in a petroleum base, the risk of
hydrocarbon pneumonitis may exceed the toxic hazard of the insec-ticide.
Gastric decontamination is therefore, generally not recommended.
·
Oils and fats (including milk) promote the intestinal
absorption of pyrethroids and should be avoided.
·
Oxygen and ventilatory asistance must be administered as
indicated.
·
Bronchospasm is treated with standard bronchodilators.
Administer beta2 adrenergic agonists. Consider use of inhaled
ipratropium and systemic corticosteroids.
·
Monitor peak expiratory flow rate, monitor for hypoxia and
respiratory failure, and administer oxygen as neces-sary. Consider systemic
corticosteroids in patients with significant bronchospasm, e.g. prednisone 60
mg/day (adult), or 1 to 2 mg/kg/day (child).
·
Seizures can be controlled with diazepam. Consider
phenobarbitone if seizures recur after diazepam 30 mg (adults) or 10 mg
(children > 5 years).
·
If hypotensive give 500 to 2000 ml crystalloid initially (20
ml/kg in children) and titrate to desired effect (stabilisation of vital signs,
mentation, urine output); adults may require up to 6 to 10 litres/24 hours.
Central venous or pulmonary artery pressure monitoring is recommended in
patients with persistent hypoten-sion. Vasopressors such as dopamine should be
used in refractory cases unresponsive to repeated doses of adrenaline, and
after vigorous intravenous crystalloid rehydration Atropine and oximes are
contraindicated, but some investigators recommend the former for drying up
secretions.
·
Cutaneous paraesthesias are said to respond to topical
applications of vitamin E.
Related Topics