Chapter: Maternal and Child Health Nursing : Obstetric Emergencies
Placental Praevia
Placental Praevia
When placenta is partially or wholly implanted in the lower uterine segment; either anterior or posterior wall. The anterior location is less serious than the posterior. Bleeding from placenta praevia is unavoidable and inevitable due to the stretching of the lower uterine segment in later weeks of pregnancy which tears the anchoring chorionic villi. Bleeding may be slight or severe depending on how much encroachment in the lower segment. When placenta lies on the internal Os bleeding is severe during
effacement and dilatation of the cervix. Bleeding may also be precipitated by coitus. Hemorrhage of this type places mother and baby at high risk and constituted obstetric emergency.
Incidence: About 0.5% of all pregnancies more common in multigravidae.
Signs & Symptoms
1. Painless vaginal bleeding which may be continuous or intermittent during rest or sleep.
2. Occasionally is accompanied with uterine contractions.
3. Increased bleeding
4. Mal presentations may be associated – Breech Transv erse or oblique lie.
5. High presentation – Non engagement of the presentin g part.
6. Unstable lie
7. Laterally – It pushes the head to one side. Posteri orlly – Overlapses the head, pushes the head anteriority giving the impression of cephalo pelvic disproportion.
Placenta Praevia is classified into degree according to placental location known as types.
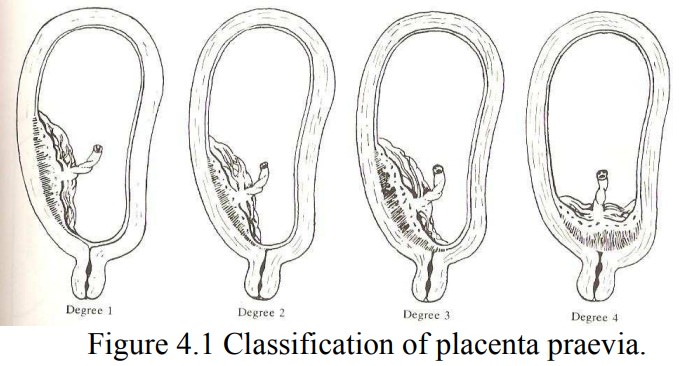
Type 1 Placenta Praevia
The majority of the placenta is in the upper uterine segment. Only a tip of the placenta tissue touches the lower segment. Bleeding is usually mild. Vaginal delivery is possible, mother and fetus are in good condition.
Type 2 Placenta Praevia
The Placenta is partially located in the lower uterine segment near the internal OS – (Marginal Placenta Praevia). A bit of the placenta touches the internal OS, vaginal delivery is possible if it anteriorly, bleeding is moderate. The fetus is usually more affected than the mother, that means fetal hypoxia is common.
Type 3 Placenta Praevia
The placenta covers the internal OS but not centrally but does not when the lower segment starts to stretch and cervix begins to efface and dilates up to 6cm. Vaginal delivery is not appropriate because the placenta precedes the fetus.
Type 4 Placenta Praevia
The placenta lies over the internal OS centrally. The OS is covered completely even at full dilalation of the cervix and torrential hemorrhage is very likely. Vaginal delivery should not be considered. Caesarean Section is essential to save the life of the mother and fetus.
Causes of placenta praevia;
1. Grande multiparity; Previous C/S,
2. Multiple Pregnancy, Previous Placenta Praevia
3. Certain fetal abnormalities.
4. Age – older mother are more at risk than younger on es.
5. Abnormal Placenta – Bipartita and succenturiate pla centae
Diagnosis
· Commonly it manifest 34-38wk though sometimes earlier.
· On general examination the woman may be clinically normal.
· On Abdominal Examination: Difficulty in identifying the fetal part on palpation.
1. Fundal height may be normal
2. Uterus is normal in consistency, no tenderness or tension
3. Fetal Heart rate may also be normal – depending on severity of bleeding.
4. Presentation may be abnormal e.g. Breech.
5. High head, oblique or Transverse lie or unstable
· On vulva Inspection Slight or severe bleeding
· Fetal movement – Excessive or slow or normal.
· Rapid respiration, Pulse – Signs of shock in the mo ther
Management
Objectives of Management;
· To control hemorrhage
· Save mother and infant’s life
Management depends on the amount of blood loss; may be active or conservative, condition of the mother or fetus, the location of the placenta, the stage of the pregnancy. In all cases Hospitalization is necessary.
Conservative Management
Mild bleeding, mother and fetus are well.
The woman will be on admission
· Bed rest until bleeding stops.
· Speculum examination to rule out incidental causes, after 24hrs of no bleeding.
· Monitor placental function by using fetal kick chart.
· Ultrasound scanning at intervals to locate placenta
· Monitor fetal growth.
· Vaginal delivery may be possible – 1 & 2 Anterior
· Remain on admission till term.
· Examination under anesthesia (EUA) – from 37weeks followed by Caesarean Section if a bulge is felt. If not the patient is induced.
Active Management
Caesarean section is necessary in cases of Severe bleeding, Types 3, 4 and 2 posterior even if fetus is dead, Bad obstetric history, elderly primip, Malpresentation – Breech. Active bleeding with induction.
Give emergency treatment
· Resuscitate
· Prepare for EUA and C/S
· C/S if fetal heart is present in respective of gestational age. In a hospital with facilities for special care of preterm.
i. I.V. infusion of 5% Dextrose saline
ii. Blood transfusion – O- negative blood.
Hysterectomy if bleeding becomes uncontrollable to save the woman’s life.
Complication
1. Post partum hemorrhage due to atony of the uterus
2. Maternal shock from blood loss (hypovolaemia)
3. Maternal death maternal mortality
4. Fetal hypoxia due to placenta separation
5. Fetal death 5-15% - usually fresh still birth
6. Placenta acreta, (in up to 15% cases)
7. Anesthetic & surgical complications.
Related Topics