Chapter: Paediatrics: Endocrinology and diabetes
Paediatrics: Rickets
Rickets
A disorder of the growing skeleton
due to inadequate mineralization of bone as it is laid down at the epiphyseal
growth plates. There is a char-acteristic widening of the ends of long bones
and characteristic radiology. Osteomalacia
occurs when there is inadequate mineralization of mature bone. Both rickets and osteomalacia may
be present at the same time.
Causes
Malnutrition and calcium
deficiency are common causes worldwide. Vitamin D deficiency is rare in
developed countries, although inadequate exposure to sunlight and exclusive
breastfeeding of 6ŌĆō12mths during infan-cy are well recognized causes.
Calcium deficiency
Dietary;
malabsorption.
Vitamin D
┬Ę Vitamin
D deficiency: dietary;
malabsorption; lack of sunlight; iatrogenic
(drug-induced, e.g. phenytoin therapy).
┬Ę Defect
in vitamin D metabolism: vitamin
D-dependent rickets type I (1A-hydroxylase deficiency); liver
disease; renal disease.
┬Ę Defect
in vitamin D action: vitamin
D-dependent rickets type II.
Phosphate deficiency
┬Ę Renal
tubular phosphate loss (isolated): hypophosphataemic rickets:
┬Ę X-linked;
┬Ę autosomal recessive;
┬Ę autosomal dominant.
┬Ę Acquired
hypophosphataemic rickets:
┬Ę Fanconi syndrome;
┬Ę renal tubular acidosis;
┬Ę nephrotoxic drugs.
┬Ę Reduced phosphate intake.
Clinical features
┬Ę Growth delay or arrest.
┬Ę Bone pain and fracture.
┬Ę Muscle weakness.
┬Ę Skeletal deformities:
┬Ę swelling of wrists;
┬Ę swelling of costochondral
junctions (ŌĆśrickety rosaryŌĆÖ);
┬Ę bowing of the long bones;
┬Ę frontal cranial bossing;
┬Ę craniotabes (softening of skull).
Diagnosis
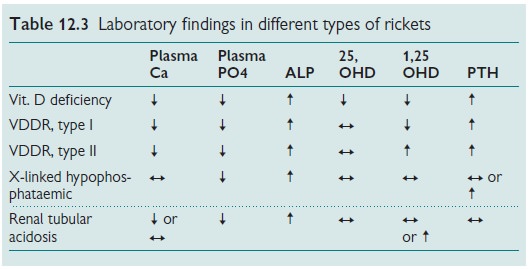
┬Ę Laboratory
(see Table 12.3):
┬Ę plasma calcium/phosphate/alkaline
phosphatase/PTH;
┬Ę vitamin D metabolites
(25-hydroxyvitamin-D3 (25 OHD)/1,25-dihydroxyvitamin-D3 (1,25 OHD)).
Radiological:
X-ray of wrists (generalized
osteopenia/widening, cupping and
fraying of metaphyses).
There are three characteristic
stages in disease progression:
┬ĘStage
1: low plasma calcium/normal plasma
phosphate.
┬ĘStage
2: normal plasma calcium (restored
due to compensatory hyperparathyroidism).
┬ĘStage
3: low plasma calcium and
phosphateŌĆöadvanced bone disease.
Stages 1 and 2 are biochemically
evident only. Stage 3 has clinical features.
Vitamin D-dependent rickets (VDDR) type I
Autosomal recessive condition. Due
to a deficiency in renal 1A-hydroxylase,
the enzyme responsible for the conversion of 25-hydroxyvitamin-D3 to 1, 25
dihydroxyvitamin-D3. The condition is due to mutations in the 1A-hydroxylase gene, P450c1A.
Patients usually present with
evidence of severe clinical rickets within the first 24mths of life.
Treatment
Requires replacement dose of 1, 25
dihydroxyvitamin-D3 (calcitriol).
Vitamin D-dependent rickets type II
Autosomal recessive condition.
This disorder is due to mutations in the vitamin D receptor gene, leading to
end-organ resistance to vitamin D. The condition is also referred to as vitamin
D resistant rickets.
Clinical, laboratory, and
radiological features are similar to those seen in vitamin D deficiency and
VDDR type I. However, a striking feature observed in the majority of patients
with VDDR-type II is sparse body hair development or total alopecia. This
finding is usually present at birth or develops during the 1st year of life
Treatment
with supraphysiological doses of
1, 25 dihydroxyvitamin-D3 (e.g. up to
60mcg/day of calcitriol) is often successful, although responses are highly
variable.
Related Topics