Chapter: Paediatrics: Nephrology
Paediatrics: Proteinuria
Proteinuria
This is defined as excessive urinary
protein excretion. Protein may be found in the urine of healthy children, and
does not exceed 0.15g/24hr.
Detection of proteinuria
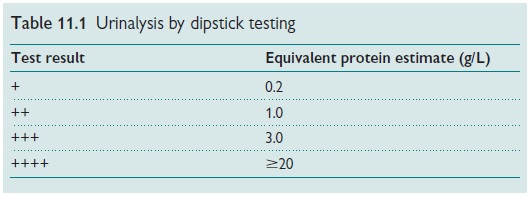
Urinalysis
Performed by dipstick testing
(Table 11.1), this is a cheap, practicable, sen-sitive method that primarily detects
albumin in the urine. It is less sensitive for other forms of proteinuria.
Urinary protein:creatinine ratio (UP:UCr)
Collection of an early morning
urine (EMU) specimen for measurement of the urinary protein to creatinine
ratio. Normal <20mg/mmol
24hr urinary protein excretion
This is the gold standard test and
requires a 24hr collection of urine to estimate urinary protein excretion.
•
Normal:
<30mg/24hr.
•
Microalbuminuria:
30–300mg/24hr.
•
Proteinuria:
>300mg/24hr.
Causes
Proteinuria may be due to benign
or pathological causes.
Non-pathological proteinuria
•
Transient.
•
Fever.
•
Exercise.
•
Urinary
tract infection (UTI).
•
Orthostatic
proteinuria (postural proteinuria). This is a common cause of referral in older
children. There is usually no history of significance and a normal examination.
Investigations reveal a normal UP:UCr ratio in early morning urine with
elevated level in afternoon specimen (may require two 12hr collections). This
is regarded as a benign finding and requires no treatment.
Pathological (persistent) proteinuria
This may be seen in a number of
renal disorders including:
•
Nephrotic
syndrome;
•
Glomerulonephritis;
•
Chronic
kidney disease;
•
Tubular
interstitial nephritis.
Investigations
Proteinuria detected on dipstick
testing should be confirmed using EMU UP:Ucr ratio. If the proteinuria is
combined with haematuria, investigations should be directed at causes of
haematuria and nephritis.
•
A
renal US scan should also be performed.
•
Patients
with persistent proteinuria detected over a period of 6–12mths should be
referred to a paediatric nephrology centre for consideration for biopsy.
Related Topics