Chapter: Paediatrics: Nephrology
Paediatrics: Chronic kidney disease
Chronic kidney disease
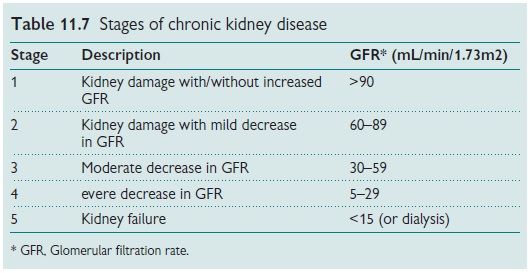
Most children with CKD are
asymptomatic until approaching chronic renal disease stage 4 (see Table 11.7).
CKD should be suspected if:
•
failure
to thrive;
•
polyuria
and polydipsia;
•
lethargy,
lack of energy, poor school concentration;
•
other
abnormalities such as rickets.
CKD: correcting common misconceptions
· Plasma creatinine can remain
normal until GFR reduced to <50%.
•
Urine
flow rate may not mean a good GFR as many children with renal dysplasia have
polyuria and nocturia.
•
Other
urinary abnormalities such as proteinuria, glycosuria can be an indicator of
tubular dysfunction.
The focus is on GFR and not plasma creatinine
•
GFR
can be formally measured by the Iohexol method or alternatively by 51Cr
EDTA or inulin methods clearance,
•
In
ordinary clinical practice GFR (mL/min/1.73m2) may be estimated
(note: less accurate in children <2yrs or >14yrs):
GFR (estimated) = 40 × height (cm)/creatinine (µmol/L).
Investigations
•
Urinalysis.
•
Blood:
FBC + iron studies if anaemic;
electrolytes/Ca/PO4/ALP/albumin;
pH/bicarbonate;
parathyroid hormone (PTH).
•
Renal
tract US.
•
Left
hand and wrist X-ray for bone age and renal osteodystrophy score.
•
ECG/echocardiography
for signs of left ventricular hypertrophy if hypertensive.
Related Topics