Chapter: Paediatrics: Nephrology
Paediatrics: Acute kidney injury: diagnosis and treatment
Acute kidney injury: diagnosis and treatment
Diagnosis
The following urinary indices may be helpful providing no diuretics have been given (Table 11.6).
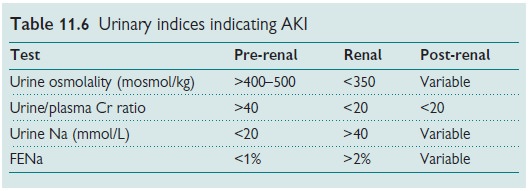
To accurately interpret fractional
excretion of sodium (FENa), patients should not have recently received
diuretics. FENa is greater than 1% (and usually greater than 3%) with acute
tubular necrosis and severe obstruc-tion of the urinary drainage.
FENa = [(UNa Ă— PCr)/(PNa Ă— UCr)] Ă— 100
where UNa and UCr
are urinary Na and creatinine, respectively, and PNa and PCr
are plasma Na and creatinine, respectively.
Treatment
Liaise with a paediatric
nephrology centre early and treat the following.
•
Hyperkalaemia
(K+ >6.5mmol/L;).
•
Metabolic
acidosis.
•
Hypertension.
•
Shock.
•
Fluid
overload.
•
Hypocalcaemia.
•
Hypo/hypernatraemia.
Specific treatment depends on the
underlying cause. However, the follow-ing general management principles apply:
•
Observations: daily weight, BP, strict fluid
input and output monitoring.
•
Fluids management: Pre-renal—fluid bolus (10mL/kg of
0.9% saline) and furosemide.
Otherwise, restrict to insensible losses (400mL/m2) + urine output.
Consider adding diuretic therapy.
Electrolytes:
monitor at least 12-hourly until
stable. K+ and PO4 restricted diet. Consider adding PO4
binder.
•
BP: treat hypertension.
•
Medications: adjust drug doses according to
level of renal impairment.
The patient may require transfer
to a paediatric nephrology centre if dialy-sis looks likely or there is
uncertainty about the diagnosis.
Indications for dialysis
The following are indications for
urgent dialysis in ARF.
•
Severe
hyperkalaemia.
•
Symptomatic
uraemia with vomiting/encephalopathy (usually urea >40mmol/L).
•
Rapidly
rising urea and creatinine.
•
Symptomatic
fluid overload, especially cardiac failure or pericardial
•
effusion.
•
Uncontrollable
hypertension.
•
Symptomatic
electrolyte problems or acidosis.
•
Encephalopathy
or seizures.
•
Prolonged oliguria: conservative regimen controls ARF,
but causes nutritional failure.
·Removal exogenous toxins or
metabolite (inborn error).
Note:
Patients with haemolytic–uraemic
syndrome should be referred as soon
as the child becomes oliguric or if urea is raised as current prac-tice is to
dialyse early to reduce neurological complications and to allow transfusion.
•
Acute dialysis—methods
•
Peritoneal
dialysis (abdominal catheter).
•
Haemodialysis
(femoral or jugular access).
•
Haemofiltration
(usually continuous veno-venous haemofiltration).
Related Topics