Chapter: Paediatrics: Growth and puberty
Paediatrics: Growth hormone deficiency: management
Growth hormone deficiency: management
GH deficiency is treated with
rhGH, which is administered as a once daily SC injection (0.7–1.0mg/m2/day
or 23–39microgram/kg/day).
· Treatment should be undertaken in
experienced centres.
· Responses to treatment (height
velocity increase) and dose adjustments should be reviewed once every 6mths.
· Catch up growth optimal if GH
therapy is started as early as possible.
Transition to GH deficiency care in adulthood
Treatment with rhGH is continued
until final adult height is achieved. At this point the GH deficiency should be
reconfirmed, particularly in those with isolated or so-called idiopathic GH
deficiency where the cause is unclear. Up to 50% of patients with the latter
may have normal GH secre-tion when retested in early adulthood. Those patients
with persisting GH deficiency should be offered the opportunity to continue
rhGH therapy (0.2–0.5mg/day). Studies have demonstrated that rhGH replacement
in adulthood may maintain lean body mass, muscle strength, and bone min-eral
density. In addition, improved quality of life has been reported with
treatment.
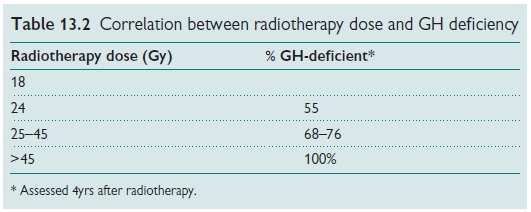
Cranial irradiation and GH deficiency
Cranial radiotherapy used in the
treatment of tumours (intracranial, face, and nasopharynx) may cause GH
deficiency. The GH axis is the most sensitive to radiotherapy, followed by the
gonadal and adrenal axes, and finally the thyroid axis, which is least
sensitive. There is a good corre-lation between radiotherapy dose and the
occurrence of hypothalamic– pituitary dysfunction (Table 13.2). Risk of
dysfunction is also related to dose fractionation (single is more toxic than
divided), and age (younger more sensitive).
Pyschosocial deprivation
Children subjected to physical or
emotional abuse may exhibit growth failure. This may be due to a reversible
inhibition of GH secretion that improves within 3–4wks of being removed from
the adverse environment. Catch-up growth is usually dramatic.
GH insensitivity syndrome
Moderate to severe short stature
may be due to GH resistance. This may be due to a defect in the GH receptor or
to a defect in post-receptor GH signalling.
Complete GH insensitivity syndrome
(GHIS) results in severe short stature. It may be inherited as an autosomal
recessive trait (Laron syn-drome). Affected individuals have high GH levels and
low circulating IGF- I levels. Exogenous rhGH administration fails to increase
IGF-I levels further (IGF-I generation test).
Related Topics