Chapter: Paediatrics: Growth and puberty
Paediatrics: Assessment of growth
Assessment of growth
Growth must be measured
accurately. Equipment used to measure weight and height must be regularly
maintained, checked, and calibrated. Ideally, growth measurements should be
carried out by someone specifically training and experienced in measurement
techniques (e.g. an auxologist). This will minimize measurement error.
Assessment of height
· From birth to age 2yrs, length is
measured horizontally using a specifically designed measuring board (e.g.
Harpenden Neonatometer). Two people need to ensure that child is lying straight
with legs extended.
· In children, aged ≥2yrs, standing
height is measured against a wall-mounted or free-standing stadiometer. A
specific technique is required, with the person measuring applying moderate
upward neck traction to the child’s head with the child looking forward in the
horizontal plane.
· Measurement of sitting height
using a modified stadiometer and calculation of the leg length (standing height
minus sitting height) allows an
estimate of upper and lower body segments and body proportion.
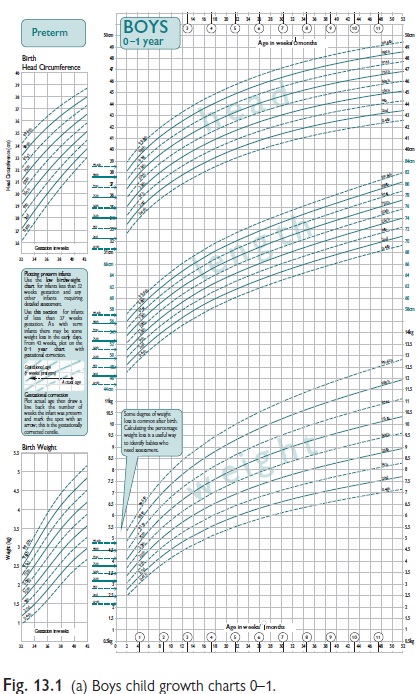
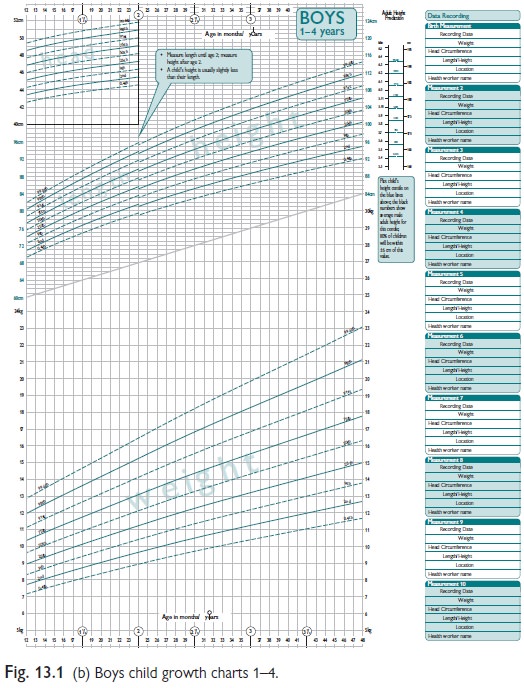
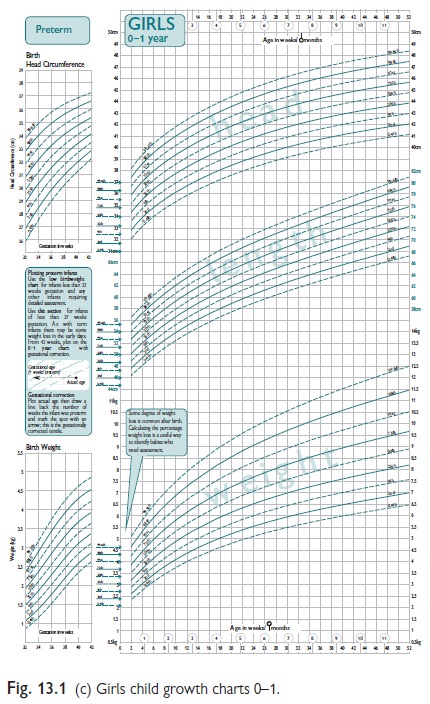
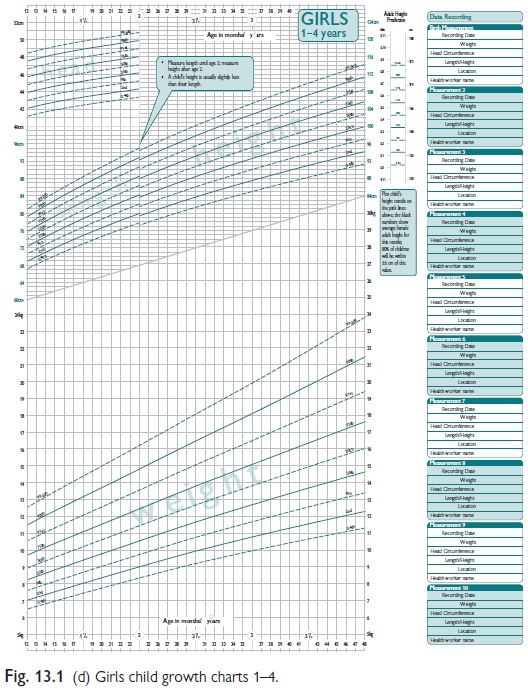
Growth data interpretation
Weight and height measurement data
should be plotted on a simple sex and age range appropriate standard growth
centile chart (e.g. the UK 1990 Growth Reference charts). A UK-WHO growth chart
for children from birth to 4yrs of age has been developed based on the WHO
child growth standards. These describe optimal growth of healthy breast-fed
children. Previous UK growth charts based on data from studies on breast- and
formula-fed children, do not reflect normal weight fluctuations of breast-fed
infants in first few weeks (see Fig. 13.1). Height measurements should be
plotted on specific population growth charts where necessary or applicable,
e.g. Turner’s syndrome; Down’s syndrome.
Single growth measurements should
not be assessed in isolation from other previous measurements. Serial
measurements are used to show a pattern of growth and to determine growth rate.
To minimize error in the assessment of growth rate, calculation of height
velocity (cm/year) should be taken from measurements a minimum of 6mths apart,
ideally using the same equipment and by the same person.
Final height and target height
Final height is the height reached
after the completion of puberty and is estimated to be achieved when growth
velocity has slowed to <2.0cm/ year. This can be confirmed by finding
epiphyseal fusion of the small bones of the hand and wrist on assessing the
bone age X-ray.
Final height is largely
genetically determined. A target height range can be estimated in each
individual from their parent’s heights, first calculating the mid-parental
height (MPH).
MPH (boys) = [(Mother’s ht (cm) +
Father’s ht (cm))/2] + 6.5cm
MPH (girls) = [(Mother’s ht (cm) +
Father’s ht (cm))/2] – 6.5cm
Target height range = MPH 9 10cm
Bone age
This is a measure of skeletal
maturation, which can be assessed by the appearance of the epiphyseal centres
of the long bones. Conventionally this is quantified from X-rays of the left
hand and wrist, with either com-pared with standard radiograph images (e.g.
Gruelich and Pyle method) or assessed using an individual bone scoring system
(Tanner–Whitehouse methods).
The difference between bone age
(BA) score and chronological age at the time of assessment may be used as an
estimation of the tempo of growth. The BA may also be used as an indicator of
the likely timing of puberty, which usually starts when BA is around 10.5yrs in
females and 11.5yrs in boys. The relationship between BA and age of onset of
menarche is more robust.
Girls usually reach skeletal
maturity at a BA of 15.0yrs and boys when BA is 17.0yrs. The BA can therefore
be used as an estimation of the remaining growth potential and can be used to
predict final adult height.
Related Topics