Chapter: Basic & Clinical Pharmacology : Adrenocorticosteroids And Adrenocortical Antagonists
Mineralocorticoids (Aldosterone, Deoxycorticosterone, Fludrocortisone)
MINERALOCORTICOIDS (ALDOSTERONE,
DEOXYCORTICOSTERONE, FLUDROCORTISONE)
The most important
mineralocorticoid in humans is aldosterone. However, small amounts of
deoxycorticosterone (DOC) are also formed and released. Although the amount is
normally insignifi-cant, DOC was of some importance therapeutically in the
past. Its actions, effects, and metabolism are qualitatively similar to those
described below for aldosterone.
Fludrocortisone, a
synthetic corticosteroid, is the most com-monly prescribed salt-retaining
hormone.
Aldosterone
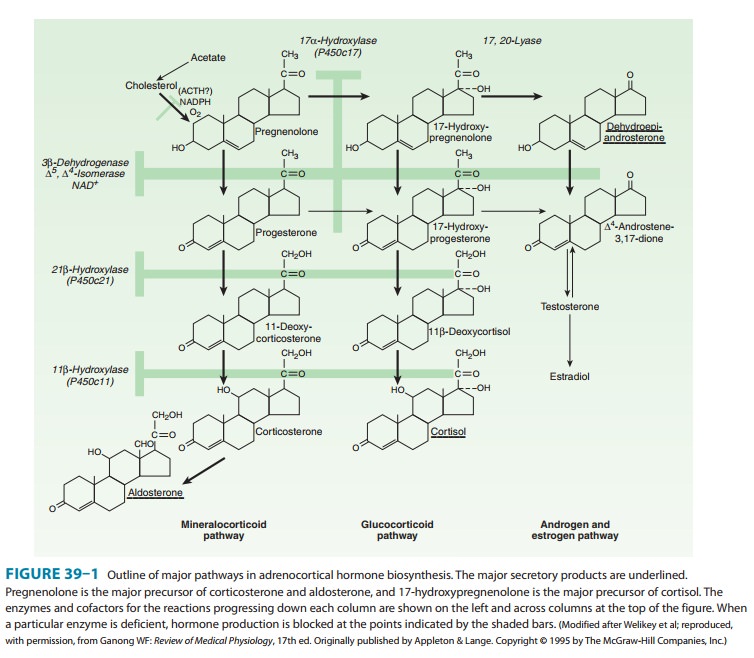
Aldosterone is
synthesized mainly in the zona glomerulosa of the adrenal cortex. Its structure
and synthesis are illustrated in Figure 39–1.
The rate of
aldosterone secretion is subject to several influ-ences. ACTH produces a moderate
stimulation of its release, but this effect is not sustained for more than a
few days in the normal individual. Although aldosterone is no less than one
third as effec-tive as cortisol in suppressing ACTH, the quantities of
aldosterone produced by the adrenal cortex and its plasma concentrations are
insufficient to participate in any significant feedback control of ACTH
secretion.
Without ACTH,
aldosterone secretion falls to about half the normal rate, indicating that
other factors, eg, angiotensin, are able to maintain and perhaps regulate its
secretion . Independent variations between cortisol and aldosterone secretion
can also be demonstrated by means of lesions in the nervous system such as
decerebration, which decreases the secretion of cortisol while increasing the
secretion of aldosterone.
A. Physiologic and Pharmacologic Effects
Aldosterone
and other steroids with mineralocorticoid properties promote the reabsorption
of sodium from the distal part of the distal convoluted renal tubule and from
the cortical collecting tubules, loosely coupled to the excretion of potassium
and hydro-gen ion. Sodium reabsorption in the sweat and salivary glands,
gastrointestinal mucosa, and across cell membranes in general is also
increased. Excessive levels of aldosterone produced by tumors or overdosage
with synthetic mineralocorticoids lead to hypokalemia, metabolic alkalosis,
increased plasma volume, and hypertension.
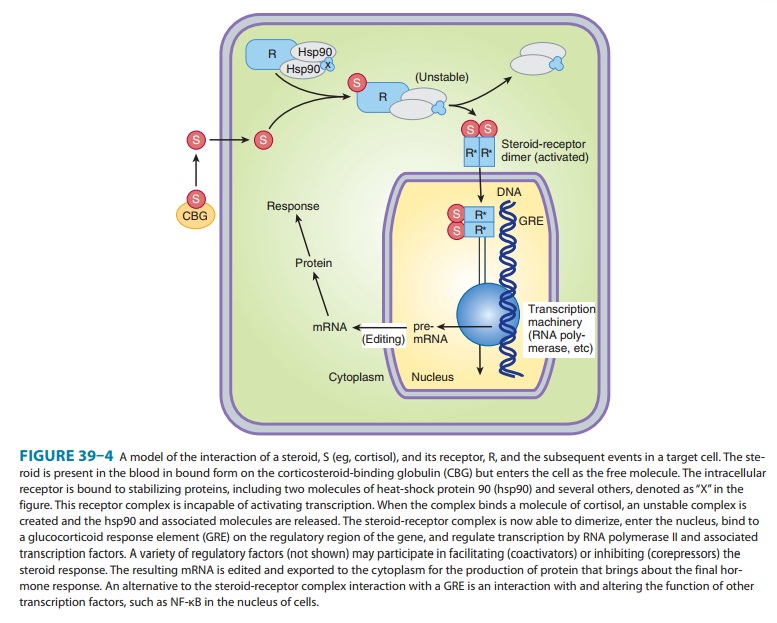
Mineralocorticoids act by binding to the mineralocorticoid receptor in the cytoplasm of target cells, especially principal cells of the distal convoluted and collecting tubules of the kid-ney. The drug-receptor complex activates a series of events similar to those described above for the glucocorticoids and illustrated in Figure 39–4. It is of interest that this receptor has the same affinity for cortisol, which is present in much higher concentrations in the extracellular fluid. The specificity for mineralocorticoids in the kidney appears to be conferred, at least in part, by the presence of the enzyme 11β-hydroxysteroid dehydrogenase type 2, which converts cortisol to cortisone. The latter has low affinity for the receptor and is inactive as a min-eralocorticoid or glucocorticoid in the kidney.
The major effect of activation of the aldosterone receptor is increased
expression of Na+/K+-ATPase
and the epithelial sodium channel (ENaC).
B. Metabolism
Aldosterone
is secreted at the rate of 100–200 mcg/d in normal individuals with a moderate
dietary salt intake. The plasma level in men (resting supine) is about 0.007
mcg/dL. The half-life of aldosterone injected in tracer quantities is 15–20
minutes, and it does not appear to be firmly bound to serum proteins.
The metabolism of
aldosterone is similar to that of cortisol, about 50 mcg/24 h appearing in the
urine as conjugated tetrahy-droaldosterone. Approximately 5–15 mcg/24 h is
excreted free or as the 3-oxo glucuronide.
Deoxycorticosterone (DOC)
DOC, which also serves
as a precursor of aldosterone (Figure 39–1), is normally secreted in amounts of
about 200 mcg/d. Its half-life when injected into the human circulation is
about 70 minutes. Preliminary estimates of its concentration in plasma are
approxi-mately 0.03 mcg/dL. The control of its secretion differs from that of
aldosterone in that the secretion of DOC is primarily under the control of
ACTH. Although the response to ACTH is enhanced by dietary sodium restriction,
a low-salt diet does not increase DOC secretion. The secretion of DOC may be
markedly increased in abnormal conditions such as adrenocortical carci-noma and
congenital adrenal hyperplasia with reduced P450c11 or P450c17 activity.
Fludrocortisone
This compound, a
potent steroid with both glucocorticoid and mineralocorticoid activity, is the
most widely used mineralocorti-coid. Oral doses of 0.1 mg two to seven times
weekly have potent salt-retaining activity and are used in the treatment of
adrenocorti-cal insufficiency associated with mineralocorticoid deficiency.
These dosages are too small to have important anti-inflammatory or antigrowth
effects.
Related Topics