Chapter: Medical Physiology: Respiratory Insufficiency-Pathophysiology, Diagnosis, Oxygen Therapy
Measurement of Maximum Expiratory Flow
Measurement of Maximum Expiratory Flow
In many respiratory diseases, particularly in asthma, the resistance to airflow becomes especially great during expiration, sometimes causing tremendous dif-ficulty in breathing. This has led to the concept called maximum expiratory flow, which can be defined asfollows: When a person expires with great force, the expiratory airflow reaches a maximum flow beyond which the flow cannot be increased any more even with greatly increased additional force. This is the maximum expiratory flow. The maximum expiratory flow is much greater when the lungs are filled with a large volume of air than when they are almost empty. These principles can be understood by referring to Figure 42–1.
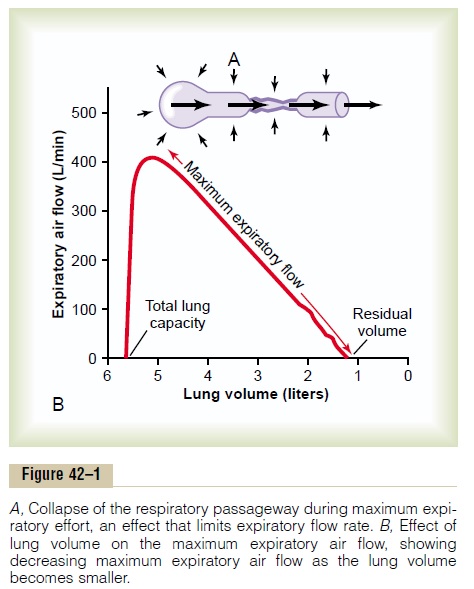
Figure 42–1A shows the effect of increased pressure applied to the outsides of the alveoli and air passage-ways caused by compressing the chest cage. The arrows indicate that the same pressure compresses the outsides of both the alveoli and the bronchioles. There-fore, not only does this pressure force air from the alveoli toward the bronchioles, but it also tends to collapse the bronchioles at the same time, which will oppose movement of air to the exterior. Once the bronchioles have almost completely collapsed, further expiratory force can still greatly increase the alveolar pressure, but it also increases the degree of bronchiolar collapse and airway resistance by an equal amount, thus preventing further increase in flow.
Therefore, beyond a critical degree of expiratory force, a maximum expiratory flow has been reached.
Figure 42–1B shows the effect of different degrees of lung collapse (and therefore of bronchiolar collapse as well) on the maximum expiratory flow. The curve recorded in this section shows the maximum expira-tory flow at all levels of lung volume after a healthy person first inhales as much air as possible and then expires with maximum expiratory effort until he or she can expire at no greater rate. Note that the person quickly reaches a maximum expiratory airflow of more than 400 L/min. But regardless of how much addi-tional expiratory effort the person exerts, this is still the maximum flow rate that he or she can achieve.
Note also that as the lung volume becomes smaller, the maximum expiratory flow rate also becomes less. The main reason for this is that in the enlarged lung the bronchi and bronchioles are held open partially by way of elastic pull on their outsides by lung structural elements; however, as the lung becomes smaller, these structures are relaxed, so that the bronchi and bron-chioles are collapsed more easily by external chest pressure, thus progressively reducing the maximum expiratory flow rate as well.
Abnormalities of the Maximum Expiratory Flow-Volume Curve. Figure 42–2 shows the normal maximum expiratory flow-volume curve, along with two additional flow-volume curves recorded in two types of lung diseases: constricted lungs and partial airway obstruction. Note that the constricted lungs have both reduced total lung capacity (TLC) and reduced residual volume (RV).
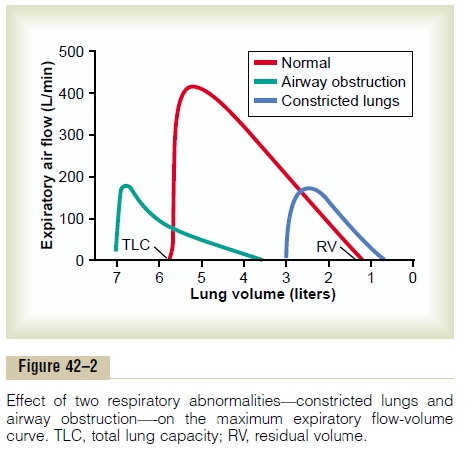
Furthermore, because the lung cannot expand to a normal maximum volume, even with the greatest pos-sible expiratory effort, the maximal expiratory flow cannot rise to equal that of the normal curve. Con-stricted lung diseases include fibrotic diseases of the lung itself, such as tuberculosis and silicosis, and dis-eases that constrict the chest cage, such as kyphosis, scoliosis, and fibrotic pleurisy.
In diseases with airway obstruction, it is usually much more difficult to expire than to inspire because the closing tendency of the airways is greatly increased by the extra positive pressure required in the chest to cause expiration. By contrast, the extra negative pleural pressure that occurs during inspiration actually “pulls” the airways open at the same time that it expands the alveoli. Therefore, air tends to enter the lung easily but then becomes trapped in the lungs. Over a period of months or years, this effect increases both the TLC and the RV, as shown by the green curve in Figure 42–2. Also, because of the obstruction of the airways and because they collapse more easily than normal airways, the maximum expiratory flow rate is greatly reduced.
The classic disease that causes severe airway obstruction is asthma. Serious airway obstruction also occurs in some stages ofemphysema.
Related Topics