Chapter: Obstetrics and Gynecology: Intrapartum Care
Labor Induction
LABOR INDUCTION
Labor can be induced when the
benefits to either the woman or the fetus outweigh those of continuing the
pregnancy. Labor induction can be achieved with intra-venous oxytocin
administration. The device used to administer oxytocin should permit precise
control of the flow rate to ensure accurate, minute-to-minute control. Various
regimens exist for stimulation of uterine con-tractions. These regimens vary in
initial dose, amount of incremental dose increase, and interval between dose
increases. Lower and less frequent dosage increases are associated with a lower
incidence of uterine hyperstimu-lation. Higher and more frequent dosage
increases may result in shorter time in labor and reduce the incidence of
chorioamnionitis and the number of cesarean deliveries performed for dystocia
(abnormal labor), but also in increased rates of uterine hyperstimulation.
Cervical
ripening may be beneficial if the cervix isunfavorable for
induction. Several techniques are avail-able. Misoprostol, a prostaglandin E
analog, is an effec-tive agent for cervical ripening and induction of labor. It
is administered vaginally. Prostaglandin E2 (PGE2) can also be administered
vaginally or intracervically. Because of the increased risk of uterine
hyperstimula-tion, both drugs are contraindicated in patients who have had a
previous cesarean delivery or previous uterine surgery.
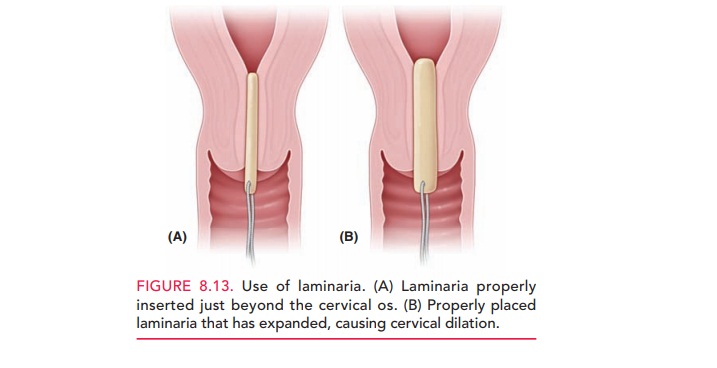
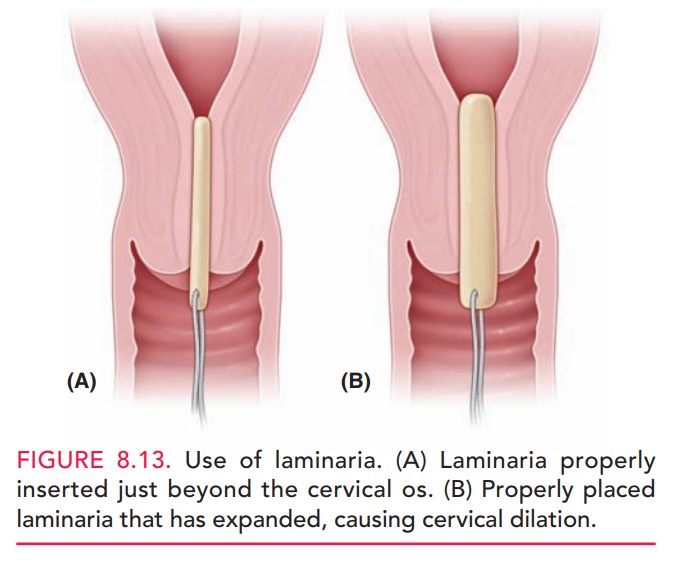
Cervical ripening also can be
accomplished with mechanical dilation with laminaria. Laminaria are
hygro-scopic rods made from the stems of the seaweed Laminariajaponica that are inserted into the internal cervical os.
Asthe rods absorb moisture and expand, the cervix is slowly dilated (Fig.
8.13). The risks associated with laminaria use include failure to dilate the
cervix, cervical laceration, inadvertent rupture of the membranes, and
infection. A synthetic form is also available. Placement of a 30 mL Foley catheter
in the cervical canal is also used for cervi-cal ripening.
Induction of labor by “stripping”
or “sweeping” the amniotic membranes is a relatively common practice. Risks
associated with this procedure include infection, bleeding from an undiagnosed placenta
previa or low-lying placenta, and accidental rupture of membranes. Artificial
rupture of membranes is another method of labor induction that may be used,
particularly when the cervix is favorable. Routine early amniotomy results in a
modest reduction in the direc-tion of labor, but may result in an increased
rate of intra-amniotic infection and cesarean delivery for fetal heart rate
abnormalities. For these reasons, routine amniotomy is not recommended.
Related Topics