Geographical Distribution, Habitat, Morphology, Life Cycle, Pathogenicity, Clinical Manifestations, Laboratory Diagnosis, Treatment, Prevention and Control - Intestinal Flagellates - Giardia Lamblia | 12th Microbiology : Chapter 8 : Medical Parasitology
Chapter: 12th Microbiology : Chapter 8 : Medical Parasitology
Intestinal Flagellates - Giardia Lamblia
Intestinal Flagellates – Giardia
Lamblia
(Also
known as Giardia duodenalis, Giardia intestinalis)
Geographical Distribution
It is the
most common protozoan pathogen and is worldwide in distribution. The disease is
very high in areas with low sanitation, especially tropics and subtropics.
Habitat
Giardia lamblia lives in the duodenum and upper jejunum of human. It is the
only protozoan parasite found in the lumen of the human small intestine.
Morphology
It exists
in two forms
• Trophozoite
and
• Cyst
Antoine van Leeuwenhoek observed and illustrated Giardia lamblia
in his own loose stool. This was the first protozoan parasite of human that is
recorded and the first to be seen under a microscope.
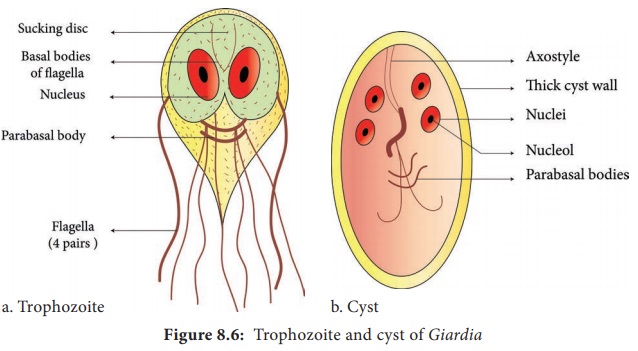
Trophozoite
The
trophozoite is in the shape of a tennis or badminton racket. It is rounded
anteriorly and pointed posteriorly. The size of the trophozoite is 14 µ long by
7µ broad. Dorsally, it is convex and ventrally, it has a concave sucking disc
which helps in its attachment to the intestinal mucosa. It is bilaterally
symmetrical. All the organs of the body are paired. Trophozoite of Giardia
possess,
• 1 pair
of nuclei
• 4 pairs of flagella
• Parabasal
body (Blepharoplast), from which the flagella arise (4 pairs)
• 1 pair of
axostyles, running along the midline
• Two sausage – shaped parabasal or median bodies
lying transversely posterior to the sucking disc
• The trophozoite is motile, with a slow
oscillation about its long axis, often resembling falling leaf (Figure 8.6a).
Cyst
It is the
infective form of the parasite. The cyst is small and oval, measuring 12 µm × 8
µm and is surrounded by a hyaline cyst wall.
Its
internal structure includes 2 pairs of nuclei grouped at one end. A young cyst
contains 1 pair of nuclei. The axostyle lies diagnonally, forming a dividing
line within cyst wall (Figure 8.6b).
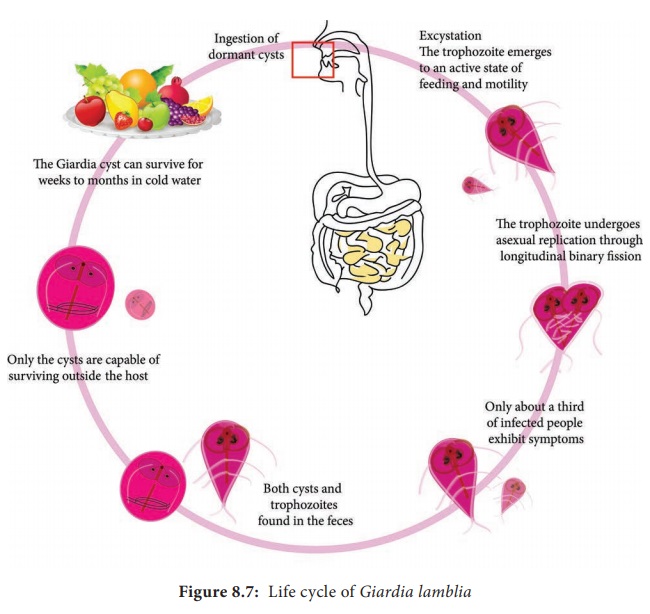
Life Cycle:
Giardia Life Cycle in Host (Human)
Infective form: Mature cyst
Mode of
transmission: Human acquires infection by ingestion of cyst in contaminated
water and food. Direct person – to person transmission occurs in children.
Transmission occurs through oral-anal and oral-genital route in sexually active
homosexual males. Within half an hour of ingestion, the cyst hatches out into
two trophozoites, which multiply by binary fission and colonize in the
duodenum. The trophozoites live in the duodenum and upper part of jejunum,
feeding by pinocytosis. When conditions in duodenum are unfavourable,
encystment occurs, usually in large intestine. Cysts are passed in stool and
remain viable in soil and water for several weeks (Figure 8.7)
Pathogenicity
Giardia lamblia does not invade the tissue, but remains attached to
intestinal epithelium by means of the sucking disc. It causes a disturbance of
intestinal function leading to malabsorption of fat
Clinical Manifestations
Incubation period is variable, but is usually about 2 weeks.
The disease is asymptomatic, but in some cases it may lead to abdominal cramps, flatulence, looseness of bowels, foul smelling stool and mild steatorrhoea (passage of yellowish and greasy stools in which there is excess of fat). The stool contains excess mucus and fat but no blood and pus. Children may develop chronic diarrhoea, malaise (discomfort), nausea, anorexia (loss of appetite for food), malabsorption of fat, vitamin A and protein. Occasionally, Giardia may colonize the gall bladder causing biliary colic and jaundice.
Laboratory Diagnosis
Specimens: Stool and blood
Examination
of stool sample: Giardiasis can be diagnosed by identification of cysts of Giardia lamblia in the formed stools and
the trophozoites and cyst of the parasite in diarrhoeal stools.
Macroscopic examination of stool: Fecal specimens containing Giardia lamblia may have an offensive
odor. It is pale coloured with fatty substance floating in water.
Microscopic
examination of stool: Cysts and trophozoites can be found in diarrheal
stools by saline and iodine wet preparations (Figure 8.8).
Serodiagnosis: Immuno chromatographic strip tests and indirect
immunofluorescence (IIF) tests are readily available. For antigen and antigen
detection ELISA, Commercially available ELISA kits detects Giardia – Specific
antigen.
Molecular methods: DNA
probes and polymerase chain reaction
(PCR) have been used to demonstrate parasitic genome in the stool specimen
Treatment
Metronidazole
and Tinidazole are the drugs of choice.
Prevention and Control
Giardiasis can be prevented and controlled by,
• Proper disposal of human faeces, maintenance of
food and personal hygiene and health education.
• After using the bathroom and before eating, the
hands should be washed thoroughly with soap and warm water. Boiling of water is
the best and effective method in killing the viable cysts.
• To reduce the risk of venereal transmission,
patients should avoid risky sexual behavior.
• No
vaccine or effective chemo prophylactic drug is available for prevention of
Giardiasis..
Related Topics