Chapter: Medicine and surgery: Principles and practice of medicine and surgery
Hypokalaemia - Fluid and electrolyte balance
Hypokalaemia
Definition
A serum potassium level of <3.5 mmol/L. Moderate hypokalemia is defined as a level of 2.5–3 mmol/L and severe as <2.5 mmol/L.
Incidence
This is a very common problem, occurring in up to 20% of inpatients.
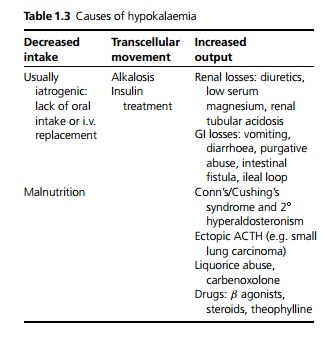
Aetiology
The most common cause is diuretics. Other causes are given in Table 1.3.
Pathophysiology
Hypokalaemia causes disturbance of neuromuscular function by altering the resting potential and slowing
repolarisation. This causes muscle weakness including the respiratory muscles and ECG changes predisposing to atrial and ventricular arrhythmias. In severe hypokalaemia sudden cardiac or respiratory arrest may occur. Other effects include the following:
· Metabolic alkalosis: In hypokalaemia there is reduced potassium secretion into the renal tubules and increased reabsorption at the H+ /K+ ATPase pump so more H+ions are lost. Hypokalaemia can both cause and maintain a metabolic alkalosis. Alkalosis also tends to promote the movement of K+ into cells, worsening the effective hypokalaemia.
· Increased digoxin toxicity: Digoxin acts by inhibition of the Na+ /K+ ATPase pump. In low-potassium states the effect of digoxin is increased, thereby increasing the risk of toxicity even at normal digoxin levels.
Clinical features
Hypokalaemia is often asymptomatic even when severe and is therefore frequently diagnosed on incidental blood testing. Symptoms include skeletal muscle weakness, muscle cramps, constipation, nausea or vomiting and polyuria. Neuropsychiatric symptoms include confusion, hallucinations, depression and even psychotic features. It is important to take a careful drug history. On examination the patient may be hypotensive and there may be evidence of cardiac arrhythmias such as bradycardia, tachycardia or ectopic beats. There may be reduced muscle strength, fasciculations or tetany. The first sign may be cardiorespiratory arrest.
Investigations
Apart from checking the serum potassium, U&Es, calcium and magnesium should be sent to look for other electrolyte abnormalities. An arterial blood gas may be indicated to look for alkalosis. The ECG shows prolonged PR interval, depressed ST segment, flattened or inverted T-wave and rarely a prominent U-wave (which appears as a long QT interval). Ventricular/atrial premature contractions or fibrillation may be seen or torsades de pointes.
Management
If severe hypokalaemia or cardiac arrhythmias are present, urgent treatment is required. Treat any life-threatening arrhythmias appropriately and give intra-venous potassium with continuous cardiac monitoring.
The highest rate of administration of potassium recommended in severe hypokalaemia is 20 mmol/h: this is higher than the usual rate of 10 mmol/h recommended in mild to moderate hypokalaemia. In asymptomatic patients with mild-to-moderate hypokalaemia oral or intravenous potassium supplements are given. The serum potassium must be rechecked frequently, e.g. every 4 hours. Any underlying cause should be looked for and managed appropriately.
Related Topics