Chapter: Ophthalmology: Eye Optics and Refractive Errors
Hyperopia (Farsightedness)
Hyperopia (Farsightedness)
Definition
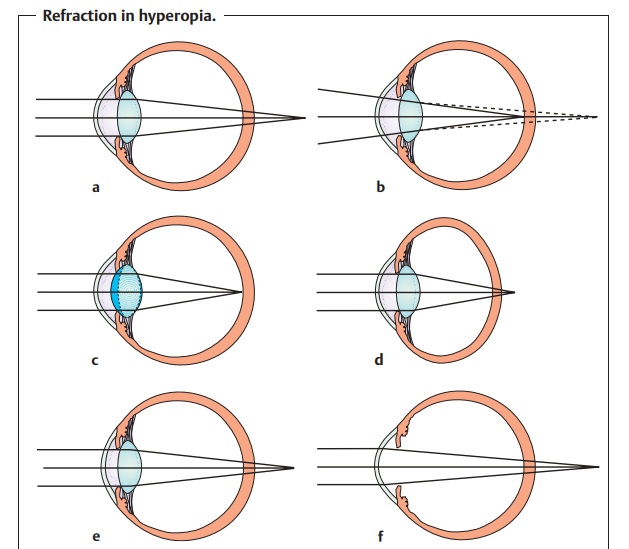
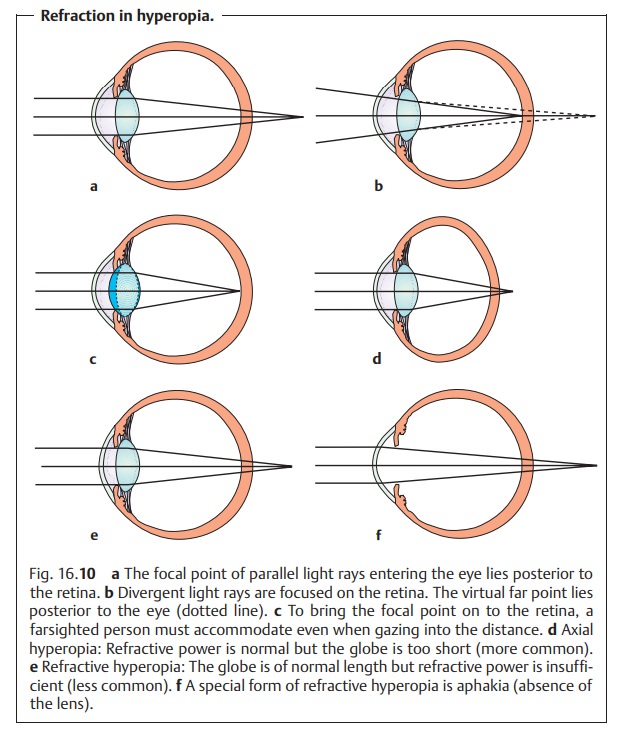
In hyperopia, there is a discrepancy between the refractive
power and axial length of the eye such that parallel incident light rays
converge at a focal pointposterior to the
retina (Fig. 16.10a).
Epidemiology:
Approximately 20% of persons between the ages of 20 and 30have refraction exceeding +1 diopters. Most newborns exhibit slight hyperopia (newborn hyperopia). This decreases during the first few years of life. In advanced age, refraction tends to shift toward the myopic side due to scleros-ing of the nucleus of the lens.
Etiology:
The mechanisms that coordinate the development of the eyeball
soas to produce optic media of a given refractive power are not yet fully
under-stood.
Pathophysiology:
In farsighted patients, the virtualfar pointof the eye liesposterior
to the retina (Fig. 16.10b).
Only convergent incident light rays can befocused on the retina (Fig. 16.10b). This is due either to an excessively shortglobe with normal
refractive power (axial hyperopia;
Fig. 16.10d) or, lessfrequently, to insufficient refractive power in a
normal-length globe (refrac-tive
hyperopia; Fig. 16.10e). Axial
hyperopia is usually congenital and ischaracterized by a shallow anterior
chamber with a thick sclera and well developed ciliary muscle.
Hyperopic eyes are predisposed to acute angle
closure glaucoma because of their shallow anterior chamber. This can be
provoked by diagnostic and therapeutic mydriasis.
Special forms of refractive hyperopia:
❖
Absence of the lens (aphakia) due to dislocation.
❖ Postoperative aphakia following cataract
surgery without placement of an intraocular lens (see Fig. 16.10).
To bring the focal point on to the retina, a
farsighted person must accommo-date even
when gazing into the distance (Fig. 16.10c). Close
objects remain blurred because the eye is unable to accommodate any further
in near vision.As accommodation is linked to convergence, this process can
result in esotropia (accommodative
esotropia or accommodative convergent stra-bismus).
Symptoms:
In young patients, accommodation can compensate for slight
tomoderate hyperopia. However, this leads to chronic overuse of the ciliary
muscle. Reading in particular can cause asthenopic
symptoms such as eye pain or headache, burning sensation in the eyes,
blepharoconjunctivitis, blurred vision, and rapid fatigue. Esotropia can also occur, as was mentioned above. As accommodation
decreases with advancing age, near vision becomes increasingly difficult. For
this reason, hyperopic persons tend to become presbyopic early.
Diagnostic considerations:
Ophthalmoscopic examination of the fundusmay reveal a slightly
blurred optic disk that may be elevated (hyperopic pseudoneuritis).
However, this is not associated with any functional impair-ments such as visual
field defects, loss of visual acuity, or color vision defects. The retina is
too large for the small eye, which leads to tortuous retinal vascu-lar structures. Transitions to abnormal
forms of axial shortening, such as inmicrophthalmos, are not well defined.
The ciliary muscle is chronically under
tension in slight or moderate hyperopia to compensate for the hyperopia. This overuse
of the ciliary muscle leads to a condition of residual accommodation in which
the muscle is unable to relax even after the hyperopia has been corrected with
plus lenses. This residual or latent hyperopia may be overlooked if refraction testing is per-formed without
first completely paralyzing the ciliary body with cycloplegic agents such as
cyclopentolate or atropine. The full extent of hyperopia includes both this
residual hyperopia and clinically manifest hyperopia.
In the presence of asthenopic symptoms of
uncertain origin, refraction testing under cycloplegia is indicated to rule out
latent hyperopia.
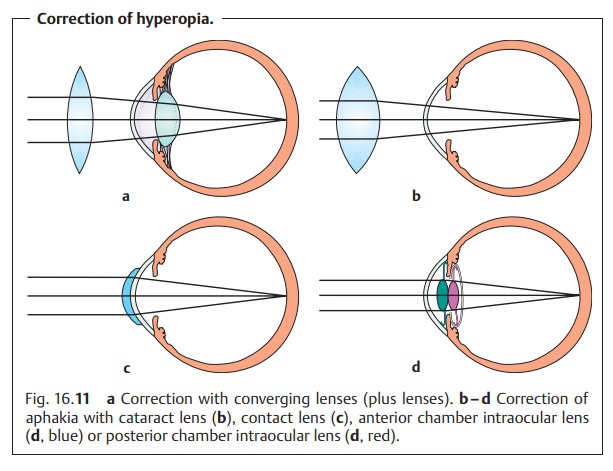
Treatment:
The insufficient refractive power must be augmented withcon-verging lenses (plus or convex
lenses; Fig. 16.11a). A
watch-and-waitapproach is indicated with asymptomatic young patients with
slight hyper-opia. Spherical plus lenses converge parallel incident light rays
at a focal point behind the lens. The refractive power (D) in plus lenses is
positive. It is equal to 1/f, where f is the focal length in meters.
Previously, biconvex or planocon-vex lens blanks were used in
the manufacture of corrective lenses. However,these entailed a number of
optical disadvantages. The optical aberrations of the positive meniscus lenses used today are comparatively slight.
The clinician should determine the total degree of hyperopia present (see Diagnostic considerations) prior to prescribing corrective lenses. The second step is to prescribe the strongest plus lens that the patient can tolerate without compromising visual acuity. Care should be taken to avoid overcor-rection. This will compensate for the manifest component of the hyperopia. If the patient wears these corrective lenses permanently, then with time it will also become possible to correct the latent component (see Diagnostic considerations). This is because the permanent tension in ciliary body is no longer necessary.
Prior to any correction of hyperopia,
refraction testing should be per-formed after administering cycloplegics to the
patient. The correction is then made with the strongest plus lens that the
patient can subjec-tively tolerate without compromising visual acuity.
In contrast, refraction testing to correct aphakiadoes not require cycloplegia. Here, too, plus lenses are required to correct the hyperopia. The closer the
plus lens is to the retina, the stronger its refractive power must be to
converge inci-dent lights at a point on the retina. For this reason, a cataract
lens (Fig. 16.11b) has a refractive power of about 12 diopters, a contact lens
(Fig. 16.11c) about 14 diopters, an anterior-chamber intraocular lens about
20 diopters (Fig. 16.11d), and a posterior-chamber lens about 23 diopters.
Related Topics