Chapter: Ophthalmology: Eye Optics and Refractive Errors
Eyeglass Lenses - Correction of Refractive Errors
Correction of Refractive Errors
Eyeglass Lenses
Monofocal Lenses
There are two basic types.
❖ Spherical lenses refract light equally along every axis.
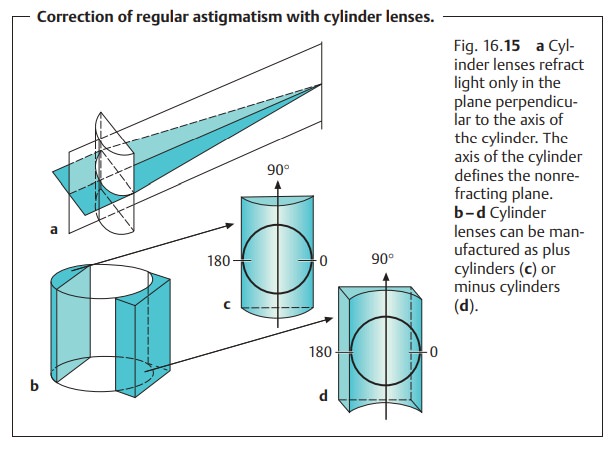
❖Toric lenses (known as cylindrical lenses) refract light only along one
axis.Spherical and toric lenses can be combined where indicated.
The refractive power of the
lenses is measured
manually or automatically with an optical interferometer. The measured
refraction is specified as spherocylindrical
combination. By convention, the specified axis of the cylin-drical lens is
perpendicular to its axis of refraction (Fig. 16.15c and d). The orientation of this axis with respect
to the eye is specified on a standardized form (Fig. 16.16).
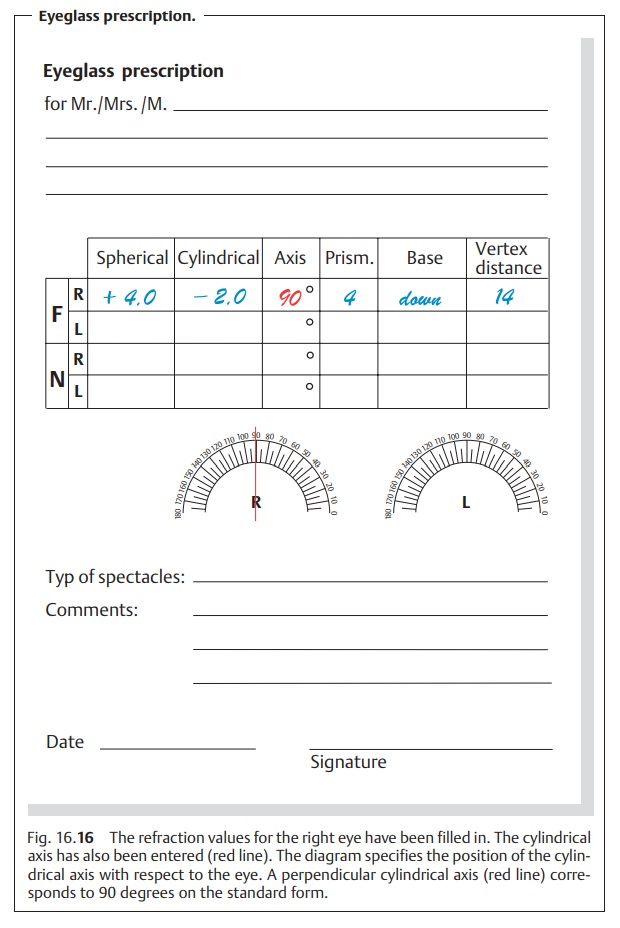
Example: + 4.00 diopters –2.00 diopters/90 degrees means that the lens
rep-resents a combination of converging lens (+ 4 diopters) and cylindrical
lens (–2 diopters) with its axis at 90 degrees.
Eyeglass lenses exhibit typical
characteristics when moved back and forth a few inches in front of one’s eye.
Objects viewed through minus lenses appear to move in the same direction as the
lens; objects viewed through plus lenses move in the opposite direction. A
cylindrical lens produces image distortions when turned.
Multifocal Lenses
Multifocal lenses differ from the monofocal
lenses of uniform refractive power discussed in the previous section in that
different areas of the lens have different refractive powers. These lenses are
best understood as combi-nations of two
or more lenses in a single lens.
Bifocals:
Theupper and middle portion of the lensis ground for thedistancecorrection; the lower portion is ground for the near-field correction (Fig. 16.17a and b). Patients are able to view distant objects in focus and read using one pair of eyeglasses, eliminating the need to constantly change glasses. The gaze is lowered and converged to read. This portion of the lens contains the near-field correction. This near-field correction can be placed in a different part of the lens for special applications.
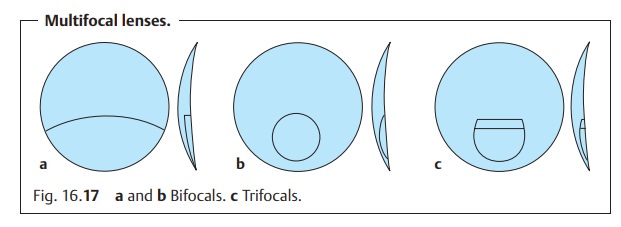
Trifocals:
These lenses include athird
refractive correctionbetween the dis-tance and near-field portions. This
intermediate portion sharply images
theintermediate field between distance vision and reading range without any
needfor accommodation (Fig. 16.17c).
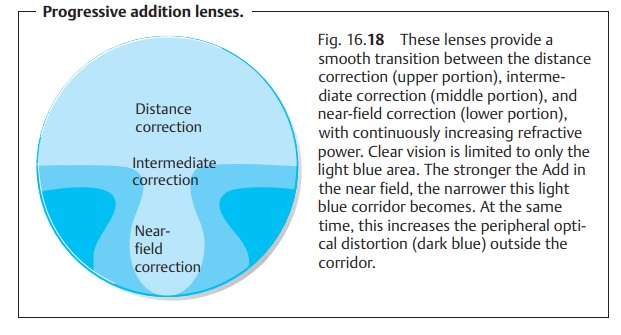
Progressive addition lenses:
These lenses were developed tominimizeabrupt image changes when the gaze moves through the
different correctionzones of the lens while maintaining
a sharp focus at every distance (Fig. 16.18).
These eyeglasses also offer cosmetic
advantages. They produce wellfocused
images in the central region but have a
high degree of peripheral astig-matism. However, many patients learn to tolerate
this peripheral distortion.
Presbyopic patients tolerate progressive addition lenses better when they still have only slight presbyopia and have not previously worn bifo-cals.
Special Lenses
The following types of lenses have been
developed for special applications:
Plastic lenses:
These lenses reduce the weight of eyeglasses where
severeametropia must be corrected. Another advantage is that these lenses are
largely shatterproof, which is why they are preferred for children. However,
they are easily scratched.
Absorption lenses:
These lenses are indicated in patients withincreased sen-sitivity to glare.
Operating motor vehicles in twilight or at
night with eyeglasses that absorb more than 20% of incident light is dangerous
because of the resulting reduction in visual acuity.
Photochromatic lenses:
These lenses darken in response to the intensity ofultraviolet
light. The lenses become darker at low temperatures than at high temperatures;
they lighten more slowly at low temperatures and more rapidly at high
temperatures. Light attenuation ranges between 15 and 50% in some lenses and
between 30 and 65% in others.
Photochromatic lenses pose problems for
patients operating motor vehicles. The lenses darken only slightly in a warm
car with the windows closed due to the lack of ultraviolet light. Dark lenses
lighten too slowly when the car enters a tunnel.
Coated lenses:
Extremely thin coatings of magnesium fluoride can beapplied to
lenses to reduce surface reflection on the front and back of the lens.
Subjective Refraction Testing for Eyeglasses
While the patient looks at vision charts, the
examiner places various combi-nations of lenses in front of the patient’s eye.
The patient reports which of two lenses produces the sharper image. The better
of the two is then compared with the next lens. This incremental method
identifies the optimal correc-tion. It is expedient to use the patient’s
objective refraction as the starting point for subjective testing. Refraction
testing is performed either with a series of test lenses from a case or with a Phoroptor, which contains many lenses that can be automatically or
manually placed before the patient’s eye.
The examination proceeds in three stages:
❖ Monocular
testing: The optimal
refraction for achieving best visual acuityis determined separately for each eye. The weakest possible minus lens is used in
myopic patients, and the strongest
possible plus lens in hyperopicpatients.
The red-green chromatic aberration test can be used for finerefraction. In this
test, the patient compares optotypes on green and red backgrounds. Fine
adjustment of refraction permits precise shifting of the focal point of the light on the retina.
Optotypes on both red and green backgrounds then appear equally sharply
defined.
❖Binocular testing: The objective of this stage is to achieve abalancebetween both eyes.
❖Near point testing: The final stage of the examination determines thepatient’s near visual acuity, and, if necessary,
the presbyopic addition (“Add”). Allowance is made for the
patient’s preferred reading and working position.
The values determined by this examination are
entered in the eyeglass pre-scription (see Fig. 16.16). The vertex distance at which refraction was per-formed is an
important additional parameter for the optician. This is the distance between the back surface of the
test lens and the anterior surface of the cornea. If the manufactured
eyeglasses have a different vertex distance,then the strength of the lenses
should be altered accordingly. This is because the optical effect of eyeglass
lenses varies according to the distance from the eye.
Before the lenses are fitted into the frame,
the distance between the pupils must be measured to ensure that the lenses are properly
centered. The centerof the lens should
be in front of the pupil. The
prismatic effects of eccentriclenses might otherwise cause asthenopic symptoms
such as headache or a burning sensation in the eyes.
To facilitate early detection of glaucoma,
intraocular pressure should be measured in any patient over the age of 40
presenting for refraction testing for eyeglasses.
Related Topics