Chapter: Microbiology and Immunology: Bacteriology: Rickettsia, Orientia Ehrlichia, and Coxiella
Genus Ehrlichia
Genus Ehrlichia
Ehrlichia are small, Gram-negative, obligate, intracellular bacillithat parasitize mononuclear and granulocytic phagocytes but not erythrocytes. The bacteria multiply in the cytoplasm of infected phagocytic cell as mulberry-like clusters called morula. The genus Ehrlichia consists of three species that cause infec-tions in human. These are (a) Ehrlichia sennetsucausing sennetsu fever, (b) Ehrlichia chaffeensis causing monocytic ehrlichiosis, and (c) Ehrlichia phagocytophila causing human granulocytic ehrlichiosis.
The genus Ehrlichia is named after the scientist Paul Ehrlich. The first case of Ehrlichia infection in humans was reported in Japan in 1954. The cases resembled glandular fever with the serum positive for antibodies against the agents of canine ehrlichiosis. The causative agent isolated from the cases was named E. sennetsu. Sennetsu is a Japanese word, meaning glandular fever.
Properties of the Bacteria
Ehrlichia are small intracellular bacteria. They stain poorly withGram stain, but stain well with Giemsa or Gimenez stain. They multiply in phagosomes of infected cells. Culture and other characteristics are same as described for rickettsia.
Pathogenesis and Immunity
Ehrlichia are intracellular pathogens. Intracellular location ofthese pathogens protects them from immune response of the host. Inside the cell, they are able to prevent fusion of phago-some with lysosome of monocytes or granulocytes, hence are not lysed by the host’s antibody response.
Clinical Syndromes
Ehrlichia species cause three clinical syndromes: (a) sennetsufever, (b) human monocytic ehrlichiosis, and (c) human granu-locytic ehrlichiosis.
◗ Sennetsu fever
Sennetsu fever is caused by E. sennetsu. The condition presents typically as an acute febrile illness and resembles glandular fever. Cervical lymphadenopathy, atypical lymphocytosis, and increase in number of peripheral mononuclear cells are the typical manifestations of the disease.
◗ Human monocytic ehrlichiosis
This condition is caused by E. chaffeensis, which infects mostly monocytes. Human diseases are associated with headache, malaise, and myalgia after 1–3 weeks of tick bite. Leukopenia, thrombocytopenia, and elevated liver enzymes are other mani-festations. Rash is found in only 20% of the patients. Mortality due to condition is less than 5% and is seen primarily in patients with immunocompromised status and also in elderly patients.
◗ Human granulocytic ehrlichiosis
This condition is caused by E. phagocytophila as well as Ehrlichiaewingii, which infect mostly granulocytes. This condition ischaracterized by a febrile illness having similar manifestations to that of human monocytic ehrlichiosis. The condition is asso-ciated with leukopenia and thrombocytopenia similar to that in human monocytic ehrlichiosis.
Epidemiology
◗ Geographical distribution
Sennetsu fever is a tick-borne disease restricted to Japan.Human monocytic ehrlichiosis is distributed mainly in the southeastern, mid-Atlantic, and south-central parts of the United States. There are areas in which lone star tick (Amblyomma americanum) are found in large numbers. Human granulocytic ehrlichiosis is distributed in the Northeast andCentral Atlantic states and in midwestern states of the United States and also in the Europe.
◗ Habitat
Like other rickettsia, Ehrlichia is found as obligate intracellular parasite in infected hosts.
Reservoir, source, and transmission of infection
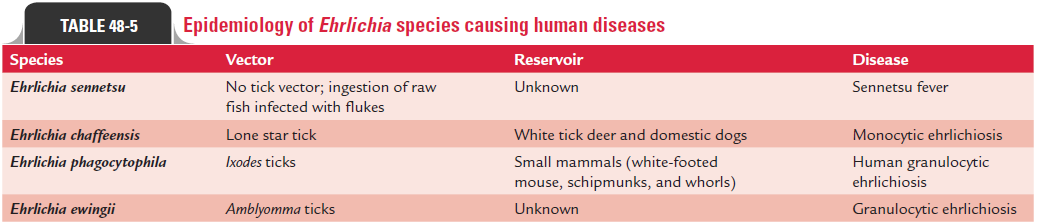
Ehrlichiosis are tick-borne diseases. Ticks are the vectors for all Ehrlichia species causing diseases in humans and ani-mals. White tick deer and domestic dogs are reservoirs for E. chaffeensis, and the bacteria are transmitted by the lone startick (A. americanum). Dogs are the vectors for E. ewingii. The lone star tick also transmits the infection. Small mammals, such as white-footed mouse, chipmunks, and whorls are the reservoirs for E. phagocytophila. Ixodes species including Ixodescapillaris, Ixodes ricinus, and Ixodes pacificus are the vectors forthe pathogen.
Reservoirs are not known for sennetsu fever. It is an exception, which is transmitted by ingestion of raw fish infected with flukes but not by ticks. The epidemiology of Ehrlichiaspecies causing human diseases is summarized inTable 48-5.
Laboratory Diagnosis
Laboratory diagnosis depends on demonstration of the patho-gen by microscopy and isolation by culture.
◗ Microscopy
Human ehrlichiosis may be diagnosed by microscopy. Giemsa-stained smear of blood films shows morulae, the intracellular form of the bacteria and is the diagnostic of the disease. However, this method has low sensitivity. Morulae are detected only in less than 10% of patients with human monocytic ehrlichiosis and in 20–80% of patients with human granulocytic ehrlichiosis.
◗ Culture
Isolation of Ehrlichia by culture is frequently used for diagnosis of ehrlichiosis.
◗ Serodiagnosis
The IFA is used to demonstrate specific antibodies in the serum by using Ehrlichia antigen prepared from the cell culture. The limitations of serological tests are that they cannot differenti-ate between E. ewingii and E. chaffeensis infections because they are antigenically closely related.
Treatment
Doxycycline is the drug of choice for treatment of human ehrlichiosis. Chloramphenicol and fluoroquinolones are not that effective.
Prevention and Control
Use of insect repellants, wearing protective clothings, etc., are the preventive measures against bites by ticks. Effective vaccine is not available.
Related Topics