Chapter: Human Neuroanatomy(Fundamental and Clinical): Internal Capsule and Commissures of the Brain
Geniculocalcarine Tract and Visual Cortex
Geniculocalcarine Tract and Visual Cortex
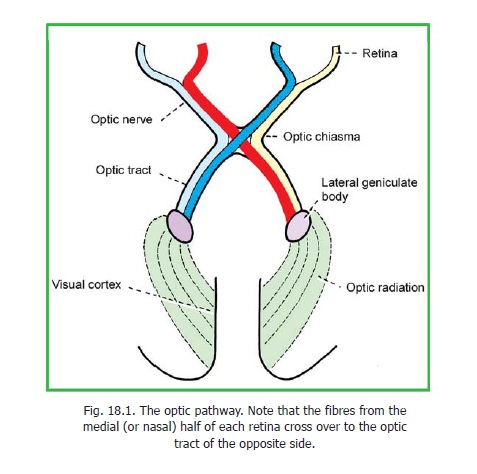
Fibres arising from cells of the lateral geniculate body constitute the geniculocalcarine tract or optic radiation. These fibres pass through the retrolentiform part of the internal capsule. The optic radiation ends in the visual areas of the cerebral cortex (areas 17, 18, 19).
Some fibres of the radiation loop forwards and downwards into the temporal lobe before turning backwards into the occipital lobe. The highest fibres may loop into the parietal lobe.
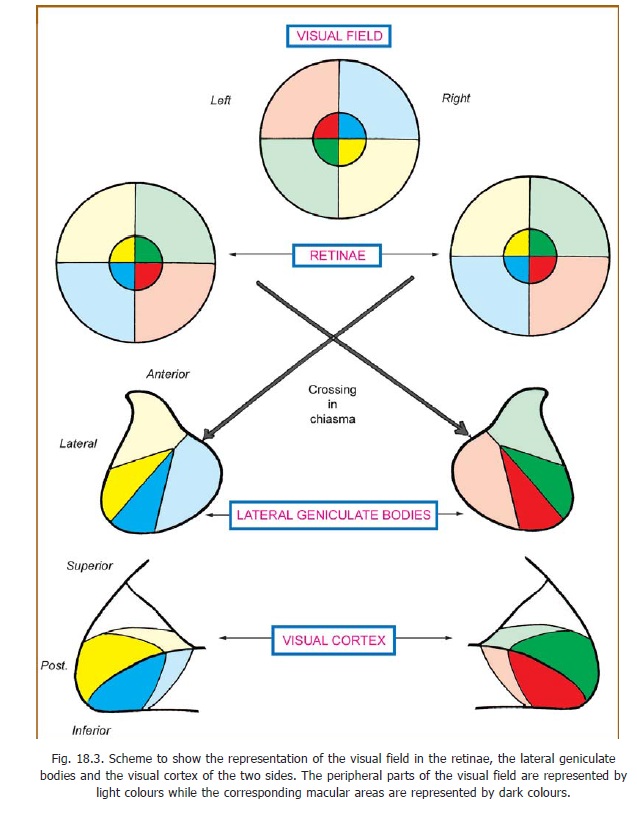
The cortex of each hemisphere receives impulses from the retinal halves of the same side (i.e., from the opposite half of the field of vision). The upper quadrants of the retina are represented above the calcarine sulcus, and the lower quadrants below it. The cortical area for the macula is larger than that for peripheral areas. It occupies the posterior part of the visual area. The cortical area for the peripheral part of the retina is situated anterior to the area for the macula.
Clinical:
Injuries to different parts of the visual pathway can produce various kinds of defects. Loss of vision in one half (right or left) of the visual field is called hemianopia. If the same half of the visual field is lost in both eyes the defect is said to be homonymous and if different halves are lost the defect is said to be heteronymous. Note that the hemianopia is named in relation to the visual field and not to the retina.
Injury to the optic nerve will obviously produce total blindness in the eye concerned. Damage to the central part of the optic chiasma (e.g., by pressure from an enlarged hypophysis) interrupts the crossing fibres derived from the nasal halves of the two retinae resulting in bitemporalheteronymous hemianopia. It has been claimed that macular fibres are more susceptible todamage by pressure than peripheral fibres and are affected first. When the lateral part of the chiasma is affected a nasal hemianopia results. This may be unilateral or bilateral. Complete destruction of the optic tract, the lateral geniculate body, the optic radiation or the visual cortex of one side, results in loss of the opposite half of the field of vision. A lesion on the right side leads to left homonymoushemianopia.
Partial injury may affect only one quadrant. The resulting condition is calledquadrantic anopia. Injury to looping fibres of the geniculocalcarine tract may lead to blindness in the upper quadrant when the lesion is in the temporal lobe; and in the lower quadrant when the lesion is in the parietal lobe.
It may be noted that in lesions of the visual pathway macular vision is often spared. This is so because of the large size of the macular area, and because some areas have a double blood supply (from posterior and middle cerebral arteries).
Lesions confined to areas 18 and 19 (peristriate and parastriate areas) may not result in loss of vision, but the patient may be unable to interpret images seen. This is visual agnosia.
Lesions anterior to the lateral geniculate body also interrupt fibres responsible for thepupillarylight reflex .
Related Topics