Chapter: Ophthalmology: Conjunctiva
General Notes on the Causes, Symptoms, and Diagnosis of Conjunctivitis
General Notes on the Causes, Symptoms, and Diagnosis of
Conjunctivitis
Definition
Conjunctivitis is an inflammatory process
involving the surface of the eye and characterized by vascular dilation,
cellular infiltration, and exudation. Two forms of the disorder are
distinguished:
❖Acute conjunctivitis. Onset is abrupt and initially unilateral with inflamma-tion of
the second eye within one week. Duration is less than four weeks.
❖ Chronic conjunctivitis. Duration is longer than three to four weeks.
Epidemiology:
Conjunctivitis is one of the most frequent eye disorders.
Etiology:
Causes of conjunctivitis may be fall into two broad categories:
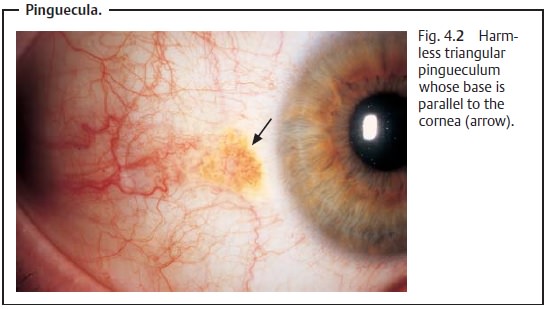
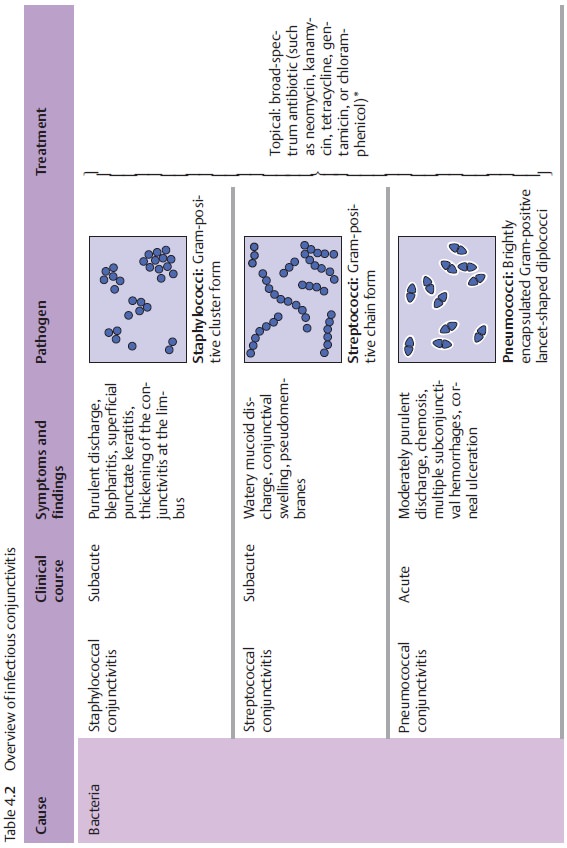
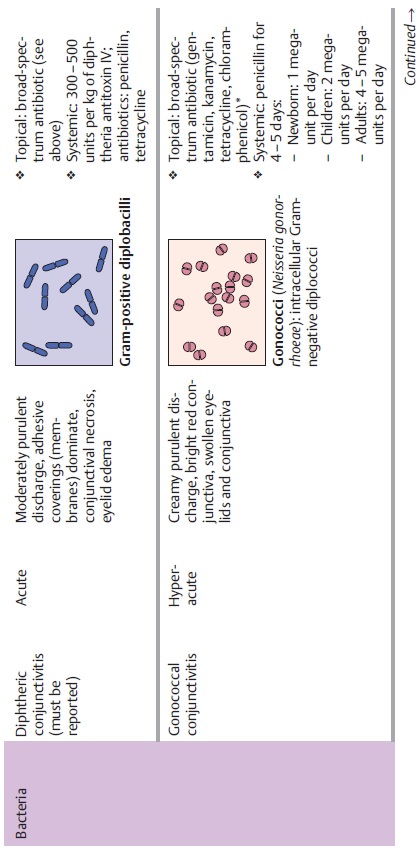
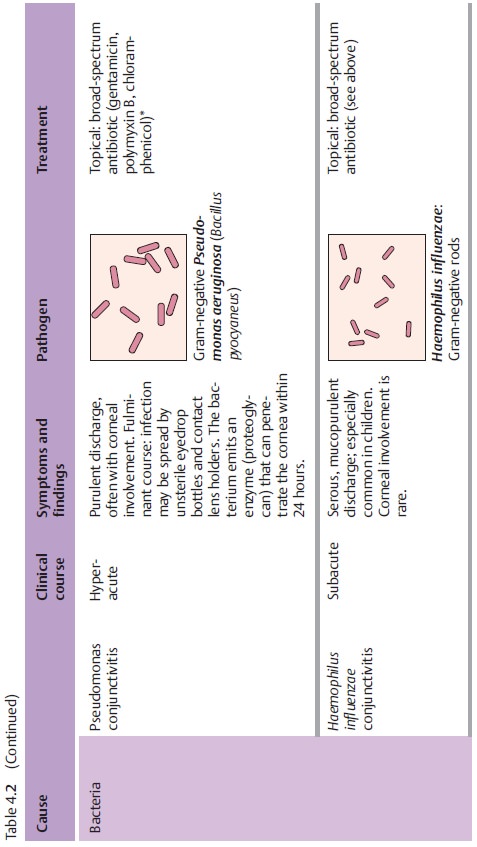
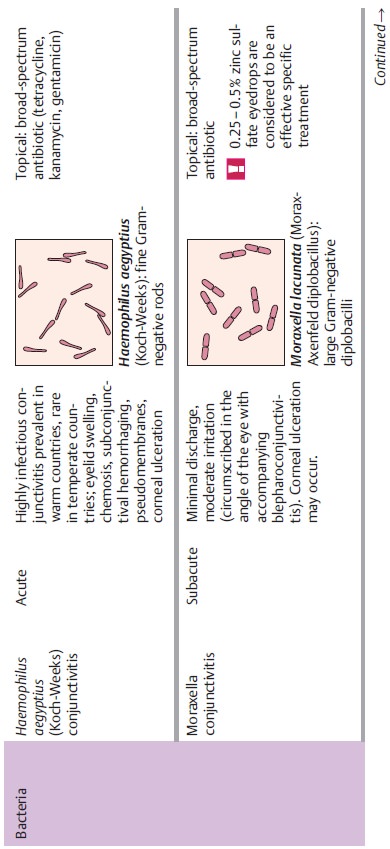
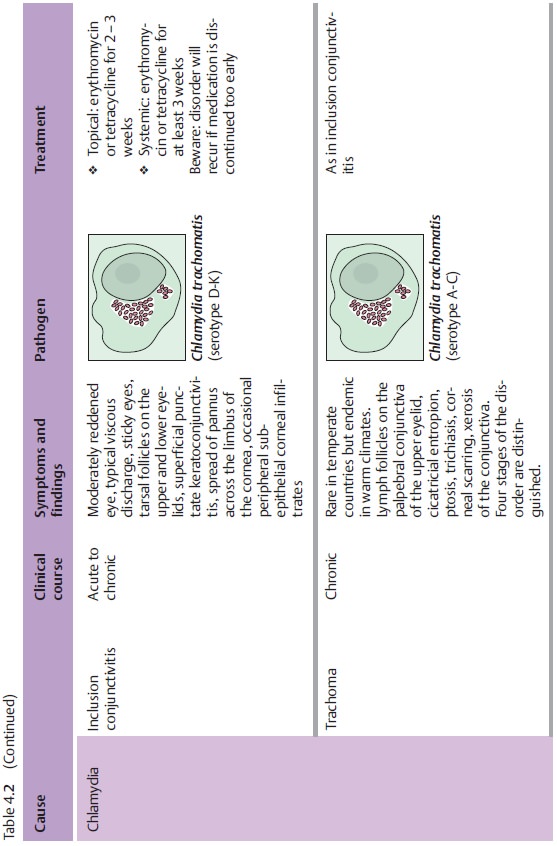
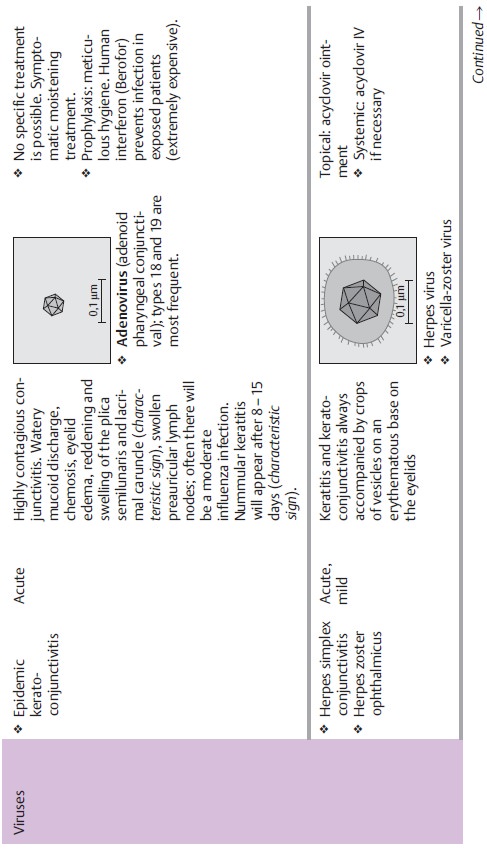
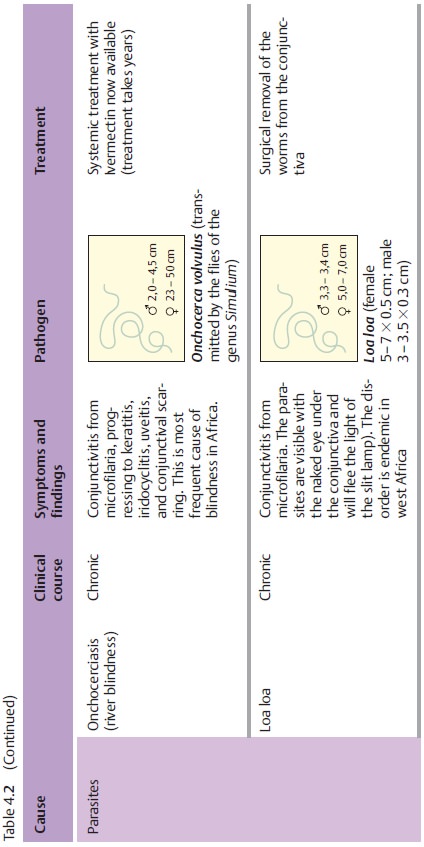
❖ Infectious(see Fig. 4.2)
–
bacterial
– viral
–
parasitic
–
mycotic
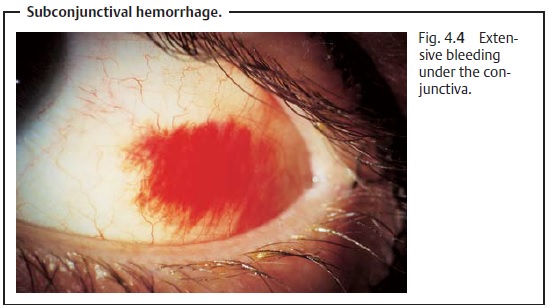
❖ Noninfectious(see Fig. 4.4)
- from a persistent irritation (such as lack
of tear fluid or uncorrected refractive error; see Fig. 4.4)
-
allergic
- toxic
(due to irritants such as smoke, dust, etc.)
- as a
result of another disorder (such as Stevens–Johnson syndrome).
Symptoms:
Typical symptoms exhibited by all patients includereddenedeyes and sticky eyelids in the morning due toincreased secretion. Any con-junctivitis also causes swelling of the eyelid, which will
appear partially closed (pseudoptosis).
Foreign-body sensation, a sensation of pressure, and a burning sensation are usually present,
although these symptoms may varybetween individual patients. Intense itching
always suggests an allergic reac-tion. Photophobia
and lacrimation (epiphora) may also
be present but can vary considerably. Simultaneous presence of blepharospasm suggests cor-neal
involvement (keratoconjunctivitis).
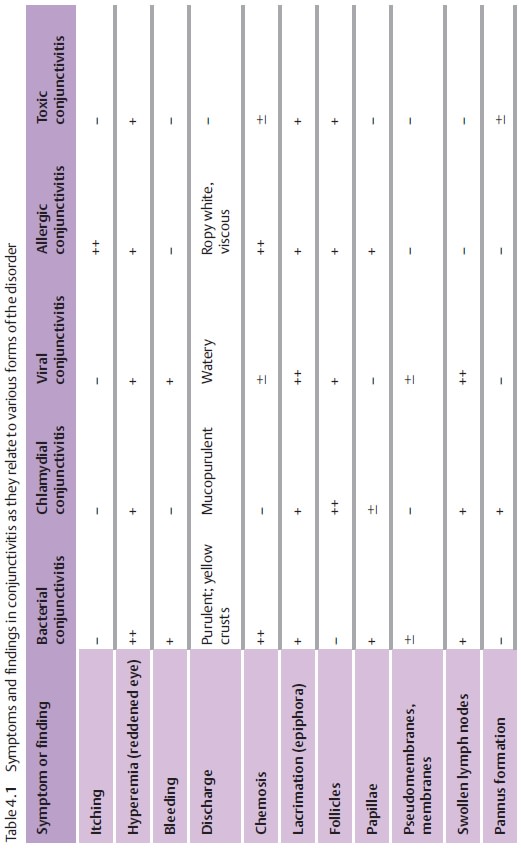
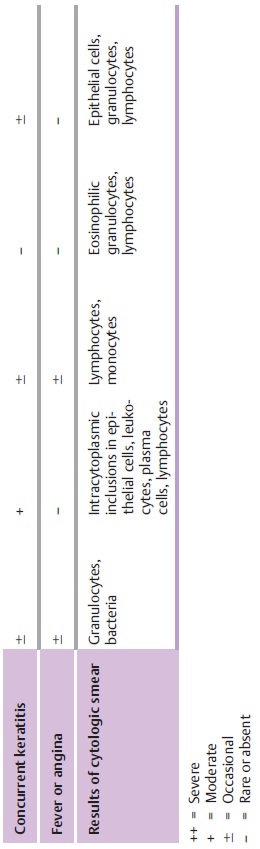
Diagnostic considerations:
There are many causes of conjunctivitis, and theclinical picture
and symptoms can vary considerably between individual patients. This makes it
all the more important to note certain characteristic findings that permit an
accurate diagnosis, such as the type of exudation, con-junctival findings, or
swollen preauricular lymph nodes (Table 4.1).
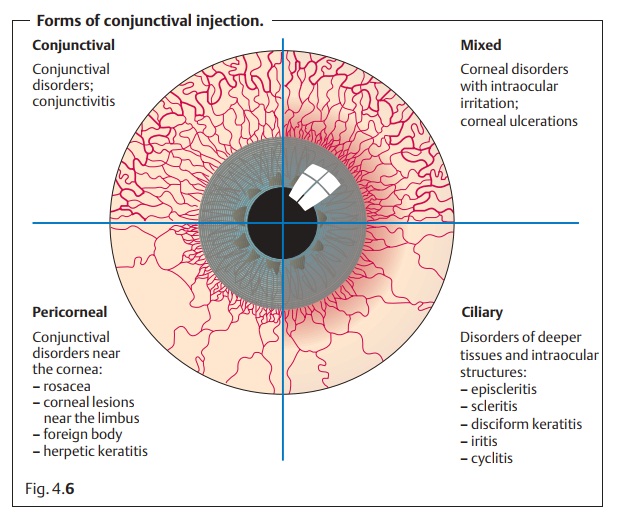
Hyperemia.Reddened eyes are a typical sign of conjunctivitis. The
conjuncti-val injection is due to increased filling of the conjunctival blood
vessels, which occurs most prominently in the conjunctival fornices. Hyperemia
is present in all forms of conjunctivitis. However, the visibility of the
hyperemic vessels and their location and size are important criteria for
differential diag-nosis. One can also distinguish conjunctivitis from other
disorders such as scleritis or keratitis according to the injection (Fig. 4.6). The following types of injection
are distinguished.
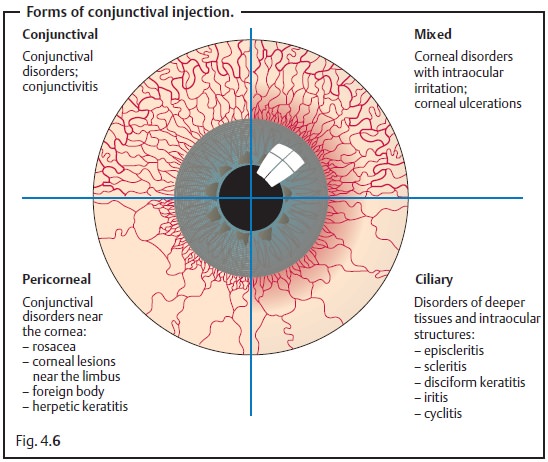
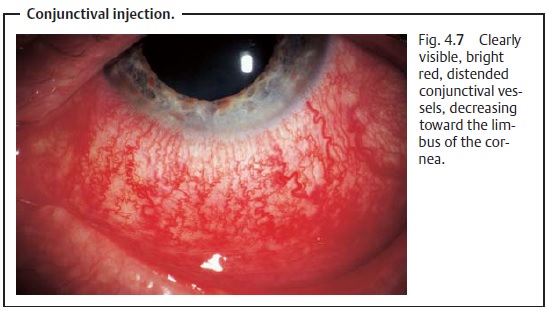
❖ Conjunctival injection (bright red, clearly visible distended vessels thatmove with the
conjunctiva, decreasing toward the limbus; Fig. 4.7).
❖ Pericorneal injection (superficial vessels, circular or circumscribed in thevicinity of the limbus).
❖Ciliary injection (not clearly discernible, brightly colored nonmobile ves-sels in
the episclera near the limbus).
❖ Composite injection (frequent).
Discharge.The quantity and nature of the exudate (mucoid, purulent,
watery,ropy, or bloody) depend on the etiology (see Table 4.1).
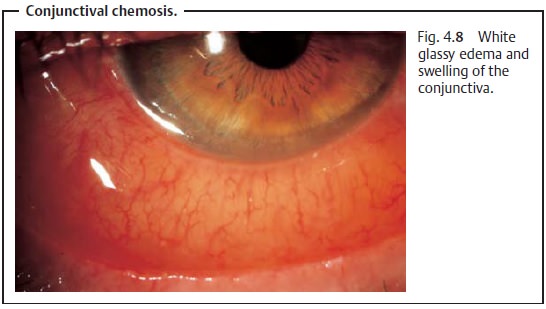
Chemosis (Fig. 4.8). This may range from the absence of any conjunctivalthickening
to a white glassy edema and swelling of the conjunctiva projecting from the
palpebral fissure (chemosis this severe occurs with bacterial and allergic
conjunctivitis).
Epiphora (excessive tearing). Illacrimation should be distinguished
fromexudation. Illacrimation is usually reflex lacrimation in reaction to a
conjunc-tival or corneal foreign body or toxic irritation.
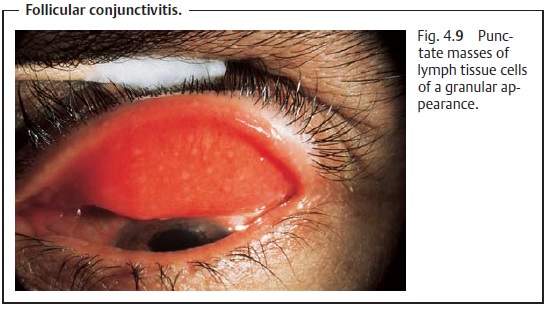
Follicle.Lymphocytes in the palpebral and bulbar conjunctiva accumulate
inpunctate masses of lymph tissue cells that have a granular appearance.
Fol-licles occur typically in viral and chlamydial infections (Fig. 4.9).
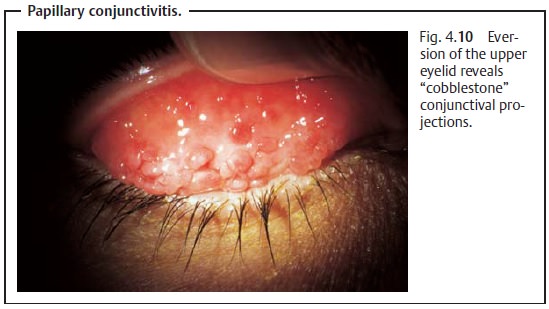
Papillae.Papillae appear as polygonal “cobblestone” conjunctival
projectionswith a central network of finely branching vessels. They are a
typical sign of allergic conjunctivitis (Fig. 4.10).
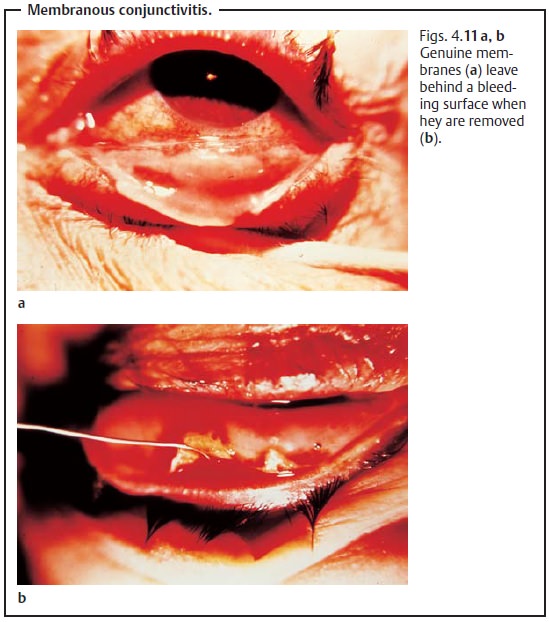
Membranes and pseudomembranes.These are conjunctival reactions tosevere infectious or toxic conjunctivitis. They form from necrotic epithelial tissue and either can be easily removed without bleeding (pseudomem-branes) or leave behind a bleeding surface when they are removed (mem-branes; Figs. 4.11a, b).
Swollen lymph nodes.Lymph from the eye region drains through thepreauricular and
submandibular lymph nodes. Swollen lymph nodes are an important and frequently
encountered diagnostic sign of viral conjunctivitis.
Pannus formation.Conjunctival or vascular ingrowth between Bowman’slayer and the
corneal epithelium in the upper circumference.
The combination and severity of individual symptoms usually provide essential information that helps to identify the respective presenting form of conjunctivitis.
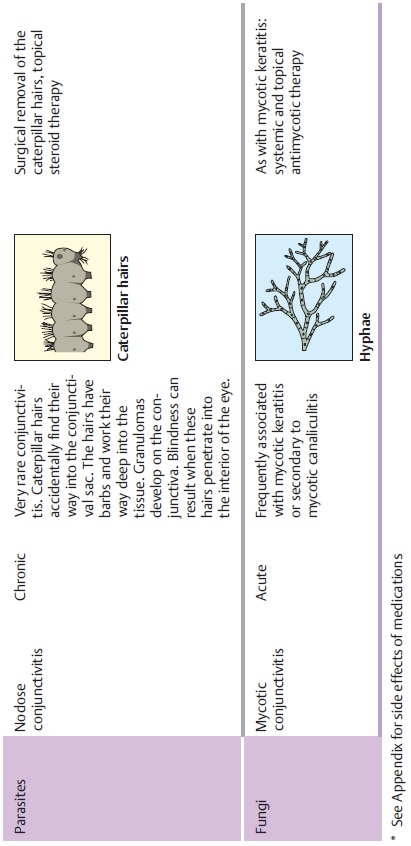
Granulomas.These are inflamed nodes of conjunctival stroma with
circum-scribed areas of reddening and vascular injection. They can occur with
sys-temic disorders such as tuberculosis or sarcoidosis or may be exogenous,
such as postoperative suture granulomas or other foreign-body granulomas.
Granulomas occur in conjunction with swollen preauricular and subman-dibular
lymph nodes in disorders such as Parinaud’s oculoglandular syn-drome.
Granulomas are not a sign of conjunctivitis in the strict sense and for that
reason have not been included as symptoms or findings in Table 4.1.
Examination methods:
Slit lamp examination.
The nature and extent of vascular injections,
discharge, conjunctival swelling, etc. are evaluated using a slit lamp.
Eyelid eversion.This is performed to examine the upper and lower eyelids forthe
presence of follicles, papillae, membranes, and foreign bodies.
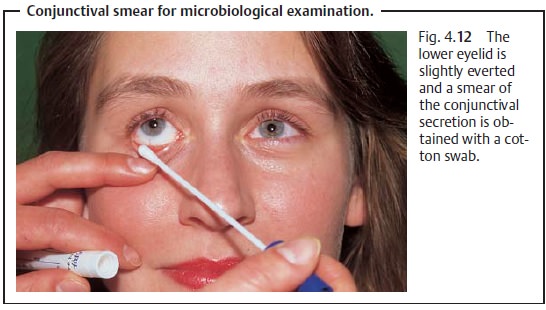
If the diagnosis is uncertain or what appears
to be bacterial conjunctivitis does not respond to antibiotics, a conjunctival smear (Fig. 4.12) should be obtained for microbiological examination to identify
the pathogen. Cotton swabs with sterile shipping tubes are commercially
available; special test kits with specific cultures are available for detecting
chlamydiae.
An antibiotic that is not effective in
treating what appears to be bacte-rial conjunctivitis should be discontinued. A
conjunctival smear should then be obtained 24 hours later. Microbiological
examination to iden-tify the pathogen is indicated for any conjunctivitis in
children.
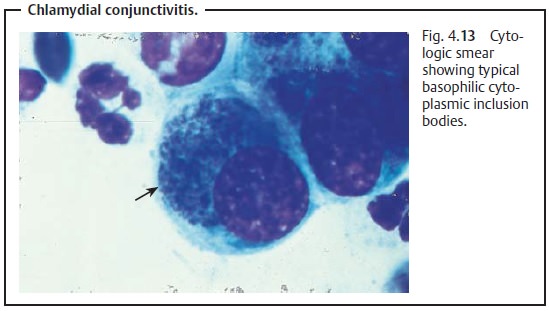
Epithelial smear.This is used to detect chlamydiae in particular and to moreclearly identify the pathogen in general. A scraping of conjunctival epithelium is smeared on a slide and dyed with Giemsa and Gram stain. Cyto-logic findings provide important information about the etiology of the con-junctivitis.
❖bacterial conjunctivitis: granulocytes with
polymorphous nuclei and bac-teria;
❖ viral
conjunctivitis: lymphocytes and monocytes;
❖chlamydial conjunctivitis (special form of bacterial conjunctivitis): com-posite findings of lymphocytes, plasma cells, and leukocytes; characteris-tic intracytoplasmic inclusion bodies in epithelial cells may also be present (see Fig. 4.13);
❖allergic conjunctivitis: findings primarily
include eosinophilic granulo-cytes and lymphocytes;
❖mycotic conjunctivitis (very rare): the Giemsa
or Gram stain will reveal the hyphae.
Irrigation.Conjunctivitis will occur occasionally in asymptomatic
dacryocys-titis or canaliculitis as a
result of continuous scattered spread of bacteria. The lower lacrimal system
should always be irrigated in the presence of inflammation that recurs or
resists treatment to verify or exclude that it is the source of the
inflammation.
Related Topics