Non Communicable Diseases - Causes, Risk factor, Signs and Symptoms, Diagnosis, Management - Gastro Intestinal Disorders | 12th Nursing : Chapter 3 : Non Communicable Diseases
Chapter: 12th Nursing : Chapter 3 : Non Communicable Diseases
Gastro Intestinal Disorders
GASTRO
INTESTINAL DISORDERS
Hernia
Cholecystitis
Appendicitis
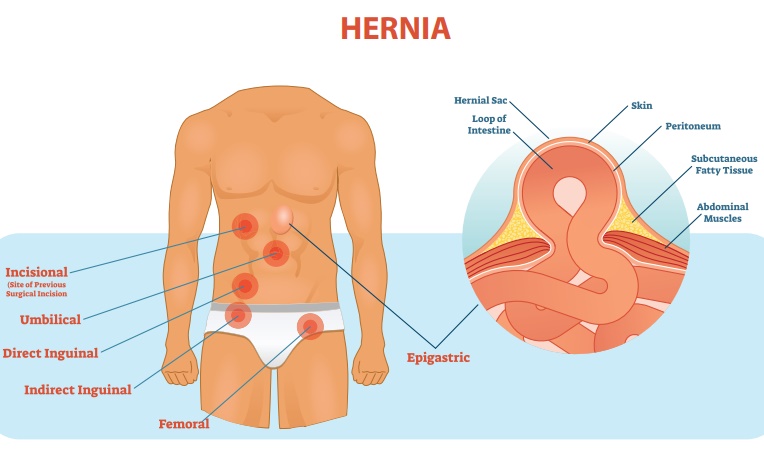
1. Hernia
A hernia is a protrusion
of an organ, tissue or structure through the wall of the cavity in which it is
normally contained.
Causes
·
Congenital weakness of the abdominal wall.
·
Acquired causes (traumatic injury, aging).
·
Increased intra-abdominal pressure due to heavy lifting, obesity,
pregnancy, straining and chronic coughing.
Types of hernia
·
Reducible: The protruding mass can be placed back into the abdominal
cavity.
·
Irreducible: the protruding mass cannot be moved back into the abdomen.
·
Incarcerated: An irreducible hernia in which the intestinal flow is
completely obstructed.
·
Strangulated: An irreducible hernia in which the blood and intestinal
flow are completely obstructed. Develops when the loop of intestine in the sac
becomes twisted or swollen and a constriction is produced at the neck of the
sac.
Classification of hernia by site
1. Inguinal hernia
Hernia into the inguinal
canal (more common in males.)
Indirect inguinal
hernia: Due to weakness of the abdominal wall at the point through
which the spermatic cord
emerges in the male and the round ligament of uterus in the female. Through
this opening the hernia extends down, the inguinal canal and often into the
scrotum or the labia.
•
Direct inguinal hernia: Passes through the posterior inguinal wall.![]()
2. Femoral hernia
Hernia into two femoral
canals appearing below the inguinal ligament that is below the groin.
3. Umbilical hernia
Protrusion of part of
the intestine at the umbilicus due to failure of umbilical orifice will close.
Occurs most often in obese women, in children and in patients with increased
intra abdominal pressure from cirrhosis and ascites.
4. Ventral (or)
incisional hernia
Hernia through the weak abdominal wall may occur after impaired healing of incision due to infection.
5. Diaphragmatic (or) hiatus hernia (or) oesophageal hernia
It is the protrusion of
a part of the stomach that slides or follows the normal path of the esophagus
and enters into the thoracic cavity through an enlarged hiatal opening.
Signs and Symptoms
·
Bulging over herniated area when patient stands or strains, and
disappears when supine.
·
Hernia tends to increase in size and recurs with intra abdominal
pressure.
·
Strangulated hernia presents with pain, vomiting, swelling of
hernia sac, peritoneal irritation and fever.
·
In hiatus hernia the patient complaints of heart burn after large
meals and during the night, food may be regurgitated.
Diagnosis
·
Based on signs and symptoms.
·
Abdominal X-rays: Reveals abnormally high level of gas.
·
Laboratory studies: Complete blood count and electrolytes may show
haeconcentration (increased hematocrit), dehydration (increased or decreased
sodium) and leucocytosis.
Management
Mechanical![]()
A truss is an appliance
with a pad and belt that is holding snugly over a hernia to prevent abdominal
contents entering the hernial sac.
Surgical management
·
Recommended to correct hernia before strangulation.
·
Strangulation of hernia is an emergency condition that
necessitates emergency laparotomy.
Herniorrhaphy
•
Removal of hernial sac, contents replaced into the abdomen, layers
of muscle and fascia sutured.
•
Laparoscopic herniorrhaphy is a possibility is often performed on
outpatient basis.
Hernioplasty
Involves reinforcement
of surturing (often with mesh) for extensive hernia repair.
Strangulated
Strangulated hernia
requires resection of ischemic bowel in addition to repair of hernia.
Nursing management
1. Achieving comfort of the patient:
•
Fit patient with truss or belt when hernia is reduced, if ordered
•
Trendelenburg’s position may reduce pressure on hernia, when
appropriate
•
Emphasize patient to wear truss under clothing and to apply
before getting out of the bed when hernia is reduced
2. Post operative care
•
Encourage the patient to splint the incision site with hand or pillow
when coughing to lessen pain and protect the site from increased
intra-abdominal pressure and wound dehiscence
•
Administer analgesics as ordered
•
Encourage ambulation as soon as permitted
•
Advise patient that difficulty in urinating is common after surgery;
promote elimination to avoid discomfort, and catheterise if necessary
3. Prevention of infection
·
Monitor the vital signs
·
Check dressings for drainage and incision for redness and swelling
·
Monitor for other signs and symptoms of infections; fever,
chills, malaise, diaphoresis
·
Administer prescribed antibiotics
4. Patient education on discharge
·
Advise that pain and scrotal swelling may be present for 24 to 48
hours after repair of an inguinal hernia
·
Apply ice intermittently
·
Elevate scrotum by using scrotal support
·
Take prescribed medication to relieve discomfort
·
Inform that heavy lifting should be avoided for 4-6 weeks
·
Athletics and extremes of extension are to be avoided for 8 to 12
weeks postoperatively
Complications
·
Bowel obstruction![]()
·
Gangrene formation
·
Wound dehiscence
2. Cholecystitis
Inflammation of the gall
bladder
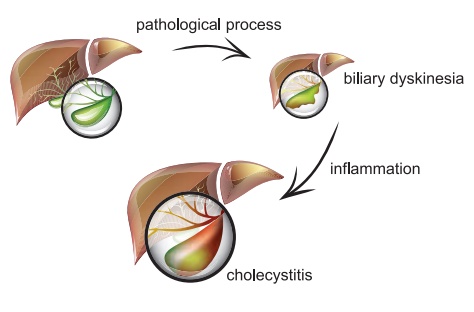
Causes
·
Exact cxauses is not known
·
Gall stones and kinking or twisting of bile duct
Risk factor
·
Sedentary life style
·
Obesity
Signs & Symptoms
·
Pain on right upper quadrant/epigastric or both
·
Nausea
·
Vomiting
·
Increased temperature
·
Mild jaundice
Investigations
·
Ultrasonography
·
Abdominal X-ray
·
Blood cell count Test (TC, DC)
Management
Medical Management
·
Hospitalization
·
Administration of antibiotics
·
Administration of parenteral analgesic
·
Insertion of nasogastric tube if patient has vomiting
·
Maintain of fluid and electrolyte balance with IV fluids
Surgical Management
·
Cholecystecotmy (Removal of Gall bladder by surgery)
Nursing management
·
History collection
·
Client symptoms should be carefully monitored
·
Check vital signs
·
Administer pain medication
·
Administer IV fluids
·
Monitor intake output chart
·
Watch for signs for dehydration
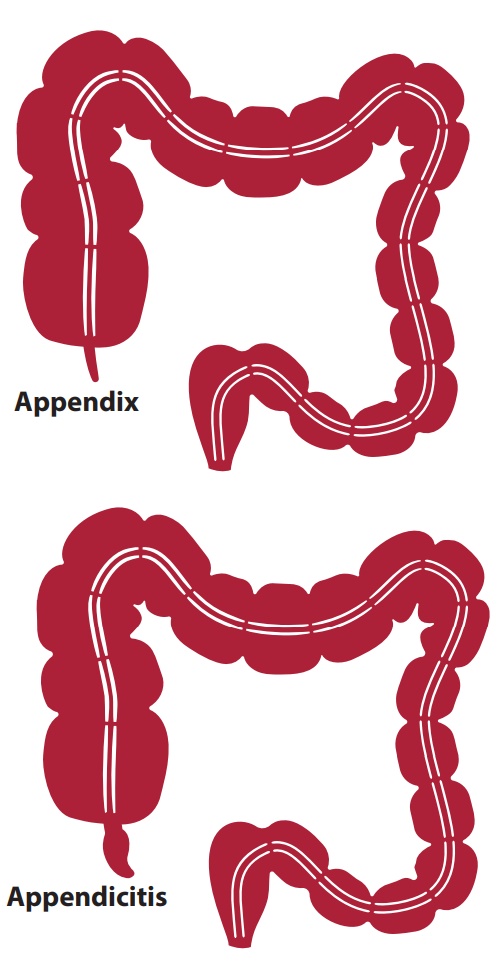
3. Appendicitis
Appendicitis is an
inflammation of the vermiform appendix caused by obstruction of the intestinal
lumen from infection, stricture, fecal mass, foreign body or tumour.
Causes
·
Obstruction of the appendix causes accumulation of mucus and
swelling leading to appendicitis.
·
Obstruction occurs due to the accumulation of faecal matter,
enlargement of lymphoid follicles, intestinal worms, and tumours.
Pathophysiology
Obstruction of the intestinal lumen is followed by edema, infection and ischemia of the appendix. As intraluminal tension develops, necrosis and perforation usually occur.
Signs and Symptoms
The typical symptoms of
acute appendicitis are
·
Severe pain in the right side of the lower abdomen.
·
Rebound tenderness at McBurney’s point.
·
Anoxia.
·
Low-grade fever.
·
Nausea and vomiting.
·
Constipation or diarrhoea occurs.
Diagnosis
·
Physical examination. Rebound tenderness at Mc Burney’s point.
·
Laboratory test: complete blood count will show
·
Leucocytosis
·
Urinalysis
·
Abdominal X-ray to visualize shadow consistent with fecalith in
appendix.
·
U.S.G. Abdomen
Management
Surgery: The standard Management
for appendicitis is surgery that involeves removal of the appendix. The
procedure is called appendectomy that can be done in two methods:
·
Laparotomy – a single incision is made to remove the appendix
·
Laparoscopic appendectomy – several small incisions are made using
special surgical tools to remove the appendix. The advantage of this surgery is
fast recovery
Complication
·
Peritonitis
·
Perforation
·
Abscess formation
Related Topics