Chapter: Ophthalmology: Ocular Motility and Strabismus
Forms of Concomitant Strabismus
Forms of Concomitant Strabismus
These essentially include the following forms:
❖ Esotropia: Inward deviation of the visual axis.
❖ Exotropia: Outward deviation of the visual axis.
❖ Hypertropia and hypotropia: Ocular deviation with one eye higher orlower than the other.
❖ Cyclotropia: This refers to the rotation of one eye around its visual axis.
Anisolated form of strabismus (i.e., one that does not occur in combination
with paralytic strabismus), this disorder is extremely rare and therefore will
not be discussed in greater detail.
Esotropia
Epidemiology:
Esotropia is one of the most commonly encountered forms
ofstrabismus.
Symptoms and diagnostic considerations:
There are three forms ofesotropia:
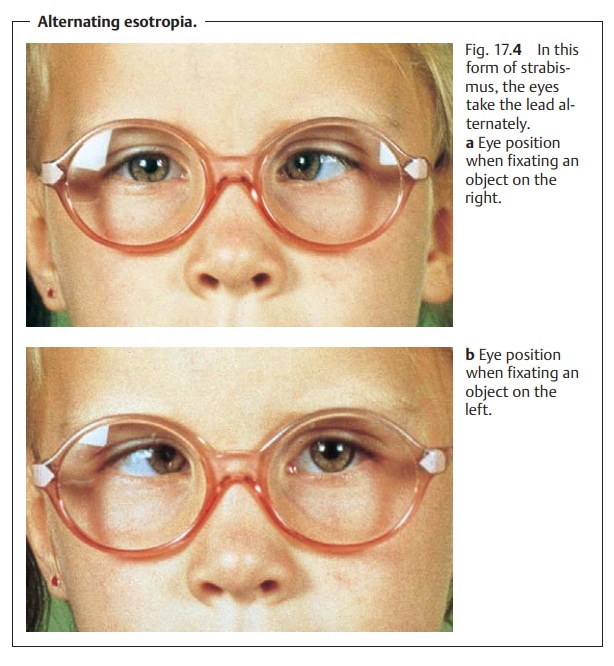
1. Congenital or infantile esotropia: Strabismus ispresent at birthordevelops within
the first six months of life.
This form is characterized by a large alternating angle of deviation (Fig. 17.4a and b), lack of binocular vision, latent nystagmus (involuntary oscillation of the eyeballs that only occurs or becomes more pronounced when one eye is covered), intermittent inclination of the head in the direc-tion of the leading eye, and additional hypertropia (primary oblique muscle dysfunction and dissociated vertical deviation).
Another motility disorder that always occurs
in infantile strabismus syn-drome is the A or V pattern deviation. This is the
result of anomalous cen-tral control,
i.e., anomalies in the pattern of nerve supply to the rectus andoblique
muscles.
❖ “A
pattern deviation” refers to an inward angle of deviation that increases in
upgaze and decreases in downgaze.
❖ “V
pattern deviation” refers to an inward angle of deviation that decreases in
upgaze and increases in downgaze.
2. Acquired strabismus: Two forms are distinguished:
❖ 1. Strabismus begins at the age of incomplete sensory development, i.e., between the
ages of one and three. Usually the disorder manifests itself at the age of two
and leads to sensory adaptation syndromes in the form of unilateral strabismus. Amblyopia is usually already present, and
cor-respondence is primarily anomalous.
❖ 2. Strabismus manifests itself between the ages of three and seven. This form of acute late strabismus with normal sensory
development is encountered far less frequently than other forms. As
binocular vision is already well developed, affected children cannot
immediately suppress the visual images of the deviating eye. As a result, they
suffer from sud-den double vision at
the onset of strabismus, which they attempt tosuppress by closing one eye. Immediate treatment is indicated to
pre-serve binocular vision. This consists of the following steps:
– Objective examination of refraction with the
pupils dilated with atropine or cyclopentolate is performed to determine
whether a refractive error is present. Clinical experience has shown that
mod-erate and severe hyperopia will be detected more frequently than in the
congenital form.
– The angle of deviation is precisely
determined and corrected with prism eyeglasses.q1w
– Surgery is indicated if eyeglass correction
fails to improve the angle of deviation within a few weeks or the eyes are
emmetropic.
Binocular vision is well developed in late
strabismus with normal sensory development. Surgery within three to six months
will allow the patient to maintain or regain stereoscopic vision.
3. Microstrabismus: This is defined as unilateral esotropia with aminimalcosmetic effect, i.e., an angle
of deviation of 5 degrees or less. As a result,microstrabismus is often
diagnosed too late, i.e., only at the age of four to six. By that time the
resulting amblyopia in the deviating eye may be severe. Another sequela of
microstrabismus is anomalous retinal corre-spondence. Binocular vision is
partially preserved despite anomalous reti-nal correspondence and amblyopia.
However, it can no longer be improved by treatment. For this reason, treatment
is limited to occlusion therapy to correct the amblyopia.
Abnormal Accommodative Convergence/Accommodation Ratio
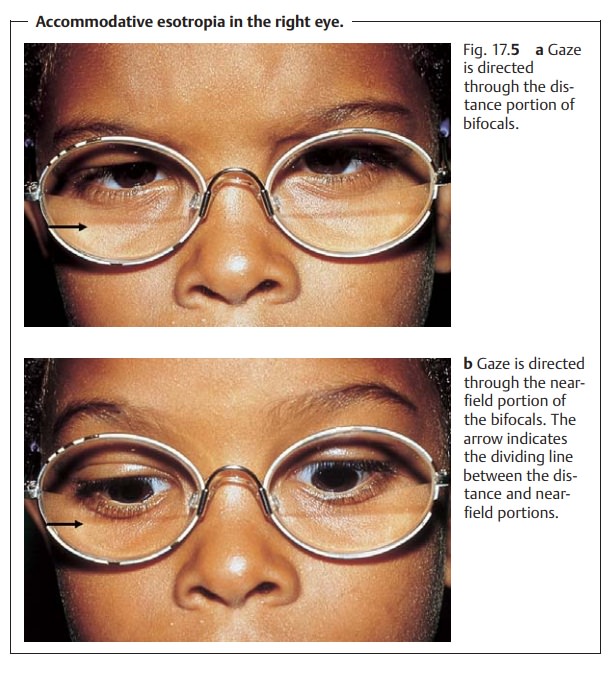
When the accommodative convergence/accommodation ratio is abnormal, the angle of deviation may fluctuate depending on whether the fixated object is far or near. For example in accommodative esotropia, the angle of deviation is larger with close objects than with distant objects. The disorder is corrected with bifocal eyeglasses, which in the case of accommodative esotropia have a strong near-field correction (Fig. 17.5a and b). A residual angle of deviation may remain despite the eyeglass correction. However, the angle of deviation may also improve to the point that the visual axes are parallel with good binocular vision.
An abnormal accommodative
convergence/accommodation ratio will cause fluctuations in ocular deviation in
near and distance fixation.
Exotropia
Exotropia (divergent strabismus) is less common than esotropia. As it is usu-ally acquired, the disorder is encountered more often in adults than in children, who more frequently exhibit esotropia. Exotropia less frequently leads to amblyopia because the strabismus is often alternating. Occasionally what is known as “panorama vision” will occur, in which case the patient has an expanded binocular field of vision. The following forms are distinguished:
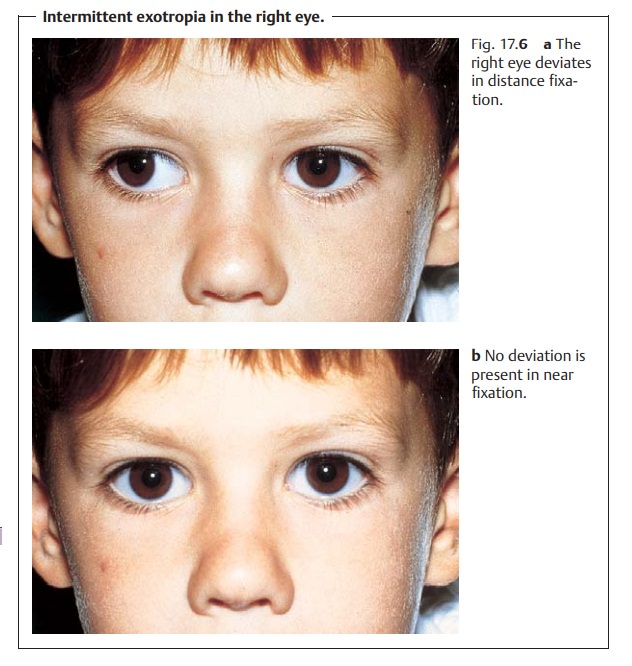
❖Intermittent exotropia. This is themost common
formof divergent stra-bismus. In intermittent exotropia, an angle of
deviation is present only when the patient gazes into the distance; the patient
has normal binocular vision in near fixation (Figs. 17.6a and b). The image
from the deviating eye is suppressed in the deviation phase. This form of
strabismus can occur as a latent disorder
in mild cases, meaning that the intermittent exotropia only becomes manifest
under certain conditions, such as fatigue.
❖ Secondary exotropia occurs with reduced visual acuity in one eye result-ing from
disease or trauma.
❖ Consecutive exotropia occurs after esotropia surgery. Often the disorder
isovercorrected.
Vertical Deviations (Hypertropia and Hypotropia)
Like A pattern and V pattern deviations,
vertical deviations are also typically caused by anomalies in the pattern of
nerve supply to the rectus and oblique muscles. Vertical deviations are usually
associated with esotropia or exotropia, for example in infantile strabismus.
Primary oblique muscle dys-function and dissociated vertical deviation are
common in this setting.
Primary oblique muscle dysfunction is characterized byupward
verticaldeviation of the adducting eye during horizontal eye movements.
Dissociated vertical deviation isalternating upward
deviation of the eyes.The respective non-fixating eye or the eye occluded
in the cover test will be elevated.
Related Topics