Chapter: Basic Radiology : The Physical Basis of Diagnostic Imaging
Fluoroscopy
Fluoroscopy
If, instead of using the light
from a fluorescent screen to blacken a film, one viewed the fluorescent screen
directly with the naked eye, then one would be performing fluo-roscopy as it
was done in the early days of medical x-ray use. Unfortunately, the image made
in this fashion was very dim, even at a high exposure rate to the patient, so
modern fluo-roscopy uses an image intensifier that amplifies the light from a
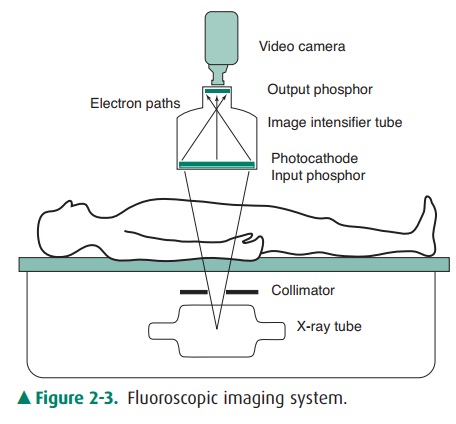
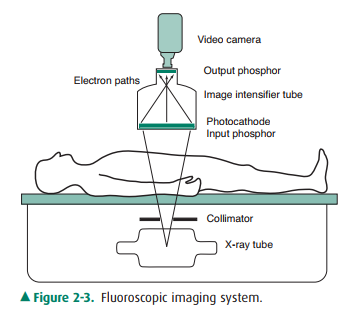
fluorescent screen. A typical fluoroscopic imaging system is shown in Figure
2-3. The image intensifier tube is an evacuated glass or metal tube with a
fluorescent screen (input phosphor) that glows with the image produced by the
x-ray pattern that exits the patient. The light from theinput phosphor causes
ejection of electrons from a photo-electric material adjacent to the input
phosphor. These elec-trons are accelerated via a high voltage (30 kV), as well
as being focused to preserve the image onto a small (1-inch di-ameter) screen
(the output phosphor), which glows with the image because of the energy
deposited by the impact of the accelerated electrons. The output phosphor glows
much more brightly than the input phosphor (about 3000 times) because of the
energy gain provided by the acceleration of the electrons and also because of
minification of the image on the output phosphor. The image on the output
phosphor can be viewed with the naked eye, usually with a series of lenses and
mirrors, but the image is more commonly viewed by fo-cusing a video camera onto
the output phosphor and viewing the image on a TV monitor via a closed-circuit
TV system. The fluoroscopic image generally has less contrast and less
resolution of fine detail than a radiographic image; however, it is clearly
convenient to view the image in real time— particularly when observing the flow
of radiopaque contrast agents ingested or injected into the body. (These
contrast ma-terials, such as iodine or barium compounds, have a higher atomic
number than soft tissue, hence, absorb more x-rays.) During fluoroscopic
examinations, the x-ray tube is typically operated below 100 kV and below 3 mA
tube current. Even so, entrance exposure rates (at the point where the x-ray
beam enters the patient) are about 2 to 5 R/min, depending on patient
thickness; hence, fluoroscopic examinations gen-erally result in significantly
higher patient exposures than do radiographic examinations.
Fluoroscopic systems generally
have an automatic bright-ness control in which the brightness of the output
phosphor is sensed by a light detector. The brightness signal from this
detector is compared to a reference level, and the difference signal is used to
instruct the x-ray generator to vary mil-liamperage or kilovoltage (or both) in
order to maintain a constant brightness at the output phosphor. For example,
after ingestion of barium in a barium-swallow examination, the barium absorbs
significantly more x-rays, and the image would tend to go dark without such a
system; however, as the brightness falls below the reference level, the
automatic brightness control causes the x-ray generator to increase the
milliamperage or kilovoltage to maintain a constant bright-ness on the monitor.
Figure 2-3. Fluoroscopic imaging system.
Related Topics