Chapter: Essential Anesthesia From Science to Practice : Clinical management : Vascular access and fluid management
Fluid requirements - Fluid management
Fluid requirements
We
calculate the intra-operative fluid requirement as follows:
·
Maintenance The 4–2–1 rule (Table3.7)provides
a guide for hourly isotonicfluid requirements.
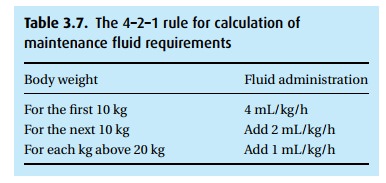
For a 70
kg man, this would amount to 40 + 20 + 50 = 110 mL/h.
·
Fasting replacement We apply the 4–2–1 rule for the duration of
fasting andreplace 50% over the first hour, then 25% over each of the next two
hours.
·
Insensible losses 2 mL/kg/h.
·
Urine output Replaced mL for mL.
·
“Third space” losses Transfer of fluid to this
sequestered, extravascular space occurs with surgical trauma, and must be
replaced with isotonic solution in the short-term: 4–8 mL/kg/h depending on the
degree of surgical trauma, e.g., peripheral operation vs. open abdomen.
·
Blood loss We replace small amounts with crystalloid (3 mL
per mL bloodlost); in larger resuscitations, colloid and/or blood is
administered 1:1 with blood loss.
Intra-operatively,
we gauge fluid status by tracking vital signs, surgical progress, urine output
(an inexact measure), and volume replacement. If the status is unclear, we may
opt for invasive monitors such as central venous or pulmonary artery pressure
monitoring (see Monitoring and Anesthesia and the cardiovascu-lar system), or
transesophageal echocardiography, which enables visualization of ventricular
filling.
Related Topics