Chapter: Essential Anesthesia From Science to Practice : Clinical management : Vascular access and fluid management
Blood replacement - Fluid management
Blood replacement
As
reviewed elsewhere (see Anesthesia and other systems: the blood), the trigger
for red cell transfusion is based not on a single laboratory value, but rather
on an assessment of the adequacy of oxygen delivery. When we deem replacement
necessary – after considering the risk : benefit ratio and the wishes of the
patient, e.g., Jehovah’s Witness – we must decide what products to order.
Blood
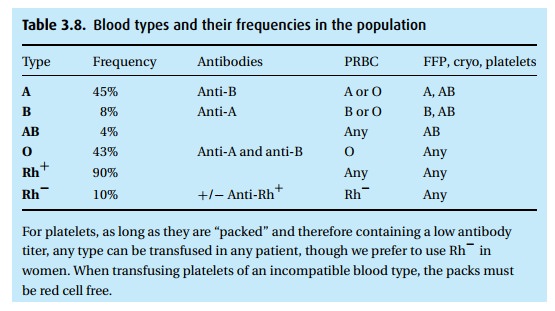
transfusions need to be ABO compatible. There are four major types, plus the
rhesus factor (Table 3.8). In an emergency,
when type-specific blood is not available, O− (“negative”) blood can serve as a “universal
donor.” Because only about 7% of the population has this blood type (and not
all happen to be blood donors), and 90% of the population is Rh+ , it is usually safe to use O+ blood in an emergency, at least in men. A
problem arises for Rh− women who might some day carry an Rh+ fetus. Maternal anti-Rh antibodies will cross
the placenta, causing potentially fatal erythroblastosis fetalis.
For
nearly all transfusions, we administer packed cells (rather than whole blood –
which enables us to collect plasma for separate infusion). For type O
transfusions, this minimizes the administration of type O serum with its anti-A
and anti-B antibodies. Once we have given more than four units of type O packed
cells, we are obliged to continue with type O transfusions because of the
admin-istered antibody load. Lacking antibodies to A, B and Rh makes type AB+ patients the universal recipient. A pity that
they are a distinct minority (3%)!
Pre-operatively, the expected need for blood transfusions covers the spectrum from: the patient will certainly not require a transfusion (no need to determine the patient’s blood type) to: we know that without several transfusions the patient cannot survive (we must prepare several units of blood for this patient). To nego-tiate the area between these extremes, we can do the following:
·
“Type and screen”: The patient’s blood is ABO and Rh typed and
screened for common antibodies (indirect Coombs test). This quick and
inexpensive test (if there is anything in today’s hospital that can be called
inexpensive) misses only about the 1% of uncommon antibodies and is therefore
usually sufficient, unless the patient has had multiple transfusions in the
past and has developed many unusual antibodies.
·
“Type and crossmatch”: The patient’s blood is typed and the
type-matched (potential) donor’s cells are exposed to the patient’s serum. This
is more involved than type and screen, costs more money and takes more time, but
readies donor blood for an immediate transfusion. We request a specific num-ber
of units to be typed and crossmatched if experience tells us to expect a large
blood loss.
When we
call the blood bank and ask for blood to transfuse, they always cross-match it
first, significantly delaying its arrival at the bedside. The ordering of
type-specific blood is an option, though there are risks of incompatibility.
Thus the time to call the blood bank is EARLY when things are not going as
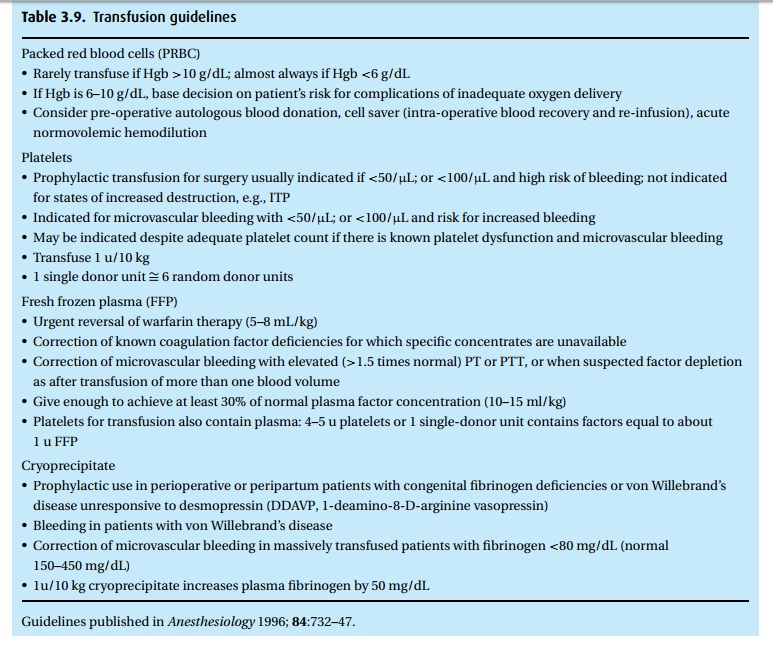
planned. Table 3.9provides some basic
transfusion guidelines, though we encourage you to check for updates regularly.
Table 3.8describes which products may be
trans-fused, based on the patient’s blood type.
Depending
on the storage medium employed, packed red blood cells come to us with a
hematocrit of 50–80%, the latter a very viscous suspension that does not infuse
well. We often dilute the PRBC unit with 50–100 mL of isotonic saline (addition
of hypotonic solutions will cause cell lysis, while calcium-containing fluids,
e.g., Ringer’s lactate, can initiate in
vitro coagulation in contact with citrated blood). Blood is stored at 1 °C
to 6 °C and should be infused through a warmer.
We use
special infusion sets that contain a filter (170-micron) to trap any clots or
other debris.
Related Topics