Chapter: Essential Anesthesia From Science to Practice : Clinical management : Vascular access and fluid management
Central venous catheterization - Vascular access
Central venous catheterization
The
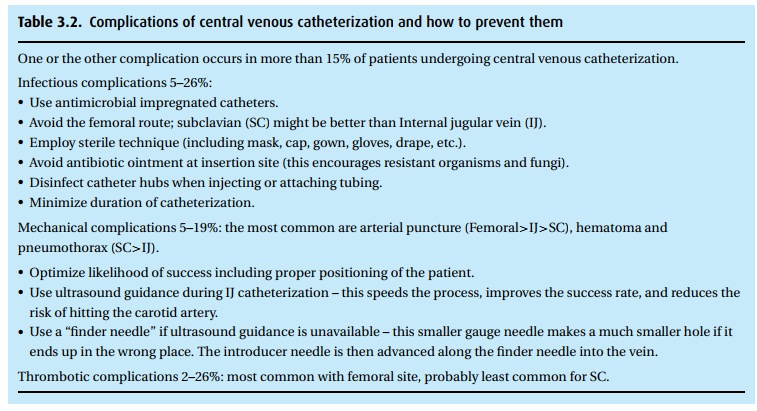
complication rate of central venous catheterization (Table 3.2) is much higher than for peripheral i.v.s,
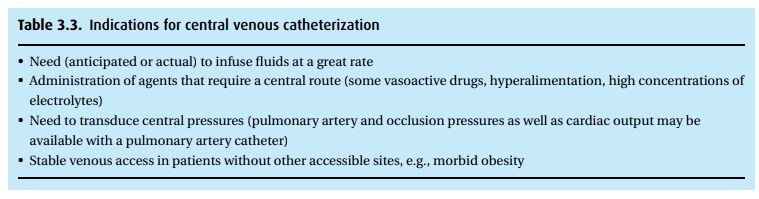
thus the first question should be whether central venous cannulation is truly
necessary (Table 3.3). When placed
emergently, for instance in a trauma patient, these catheters should be
replaced within 48 hours to reduce the risk of infection.
The next
question deals with access site. The three most common insertion sites are as
follows:
·
Femoral Probably technically the easiest (remember,
from lateral to medial,NAVEL – nerve, artery, vein, empty space, lympathics)
and quickest, with the lowest rate of serious complications (though highest
rate of minor complica-tions), but these catheters are more difficult to keep
clean and therefore more likely to be a source of infection.
·
Subclavian (SC) Once placed, this catheter location is probably
the most com-fortable for the patient. Unfortunately, it carries a significant
risk of pneumo-thorax (up to 3%), and the procedure can be very difficult when
landmarks are obscured, as in obesity.
·
Internal jugular (IJ) Anesthesiologists favor this location because
of accessibility(we’re already at the head of the patient) and the low risk of
pneumothorax. Incidentally, we prefer the right IJ over the left due to the
“straightness” of the route to the heart and because we need not worry about
the left-sided thoracic duct.
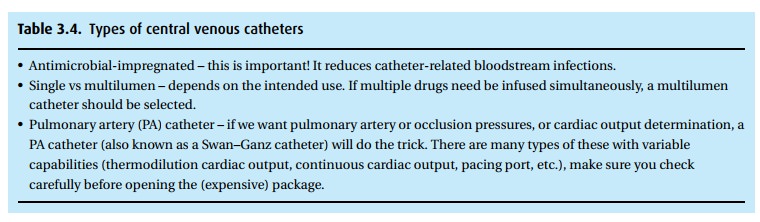
In
addition to selecting a catheter size appropriate to the patient and
indication, there are other features to consider (Table 3.4).
Because
the majority of catheters in anesthesia are placed in the IJ location in an
anesthetized patient, we will describe this technique. In an awake patient, we
would add sedation, continual reassurance, and local anesthesia.
Related Topics